You feel tired all the time. Your hair is falling more than usual. A routine blood test reveals that your hemoglobin level is low. For many people, this is the first sign of Iron Deficiency Anemia, the most common cause of Anemia worldwide and one of the most widespread nutritional deficiencies.
In this guide, we explain what iron deficiency anaemia is, why it develops, how it appears in blood test results, and when you should seek medical advice.
What Is Iron Deficiency Anemia?
Iron deficiency anemia occurs when your body does not have enough iron to produce adequate hemoglobin.
Hemoglobin is the protein inside red blood cells that carries oxygen from your lungs to every tissue and organ in your body.
Without enough of it, your cells receive less oxygen than they need — and you begin to feel the effects throughout your body.
It is the leading cause of anemia globally and, importantly, one of the most treatable conditions once correctly identified.
How Common Is It?
Iron deficiency anemia affects an estimated 1.2 billion people worldwide.
It is especially prevalent among women of reproductive age and children in South Asia, including India, where it remains a significant public health concern.
What Happens Inside Your Body?
To understand iron deficiency anemia, it helps to know how iron works.
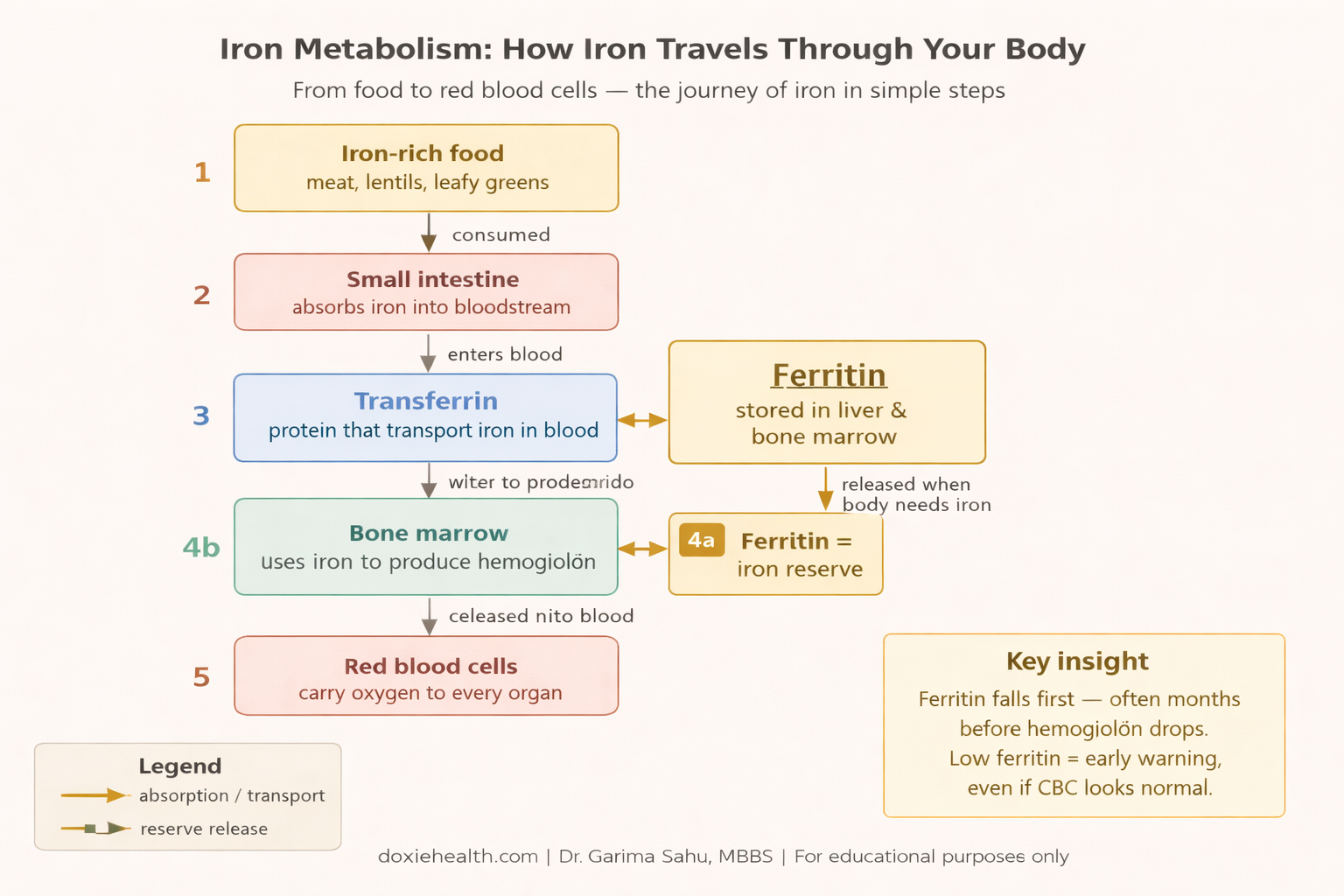
How iron travels through your body — from food to red blood cells via transferrin and ferritin. Diagram: DoxieHealth
After iron is absorbed from food in the small intestine, it is transported through the bloodstream by a protein called transferrin and stored in the liver and bone marrow as ferritin.
The bone marrow — the spongy tissue inside your bones where all blood cells are produced — uses this stored iron to build hemoglobin.
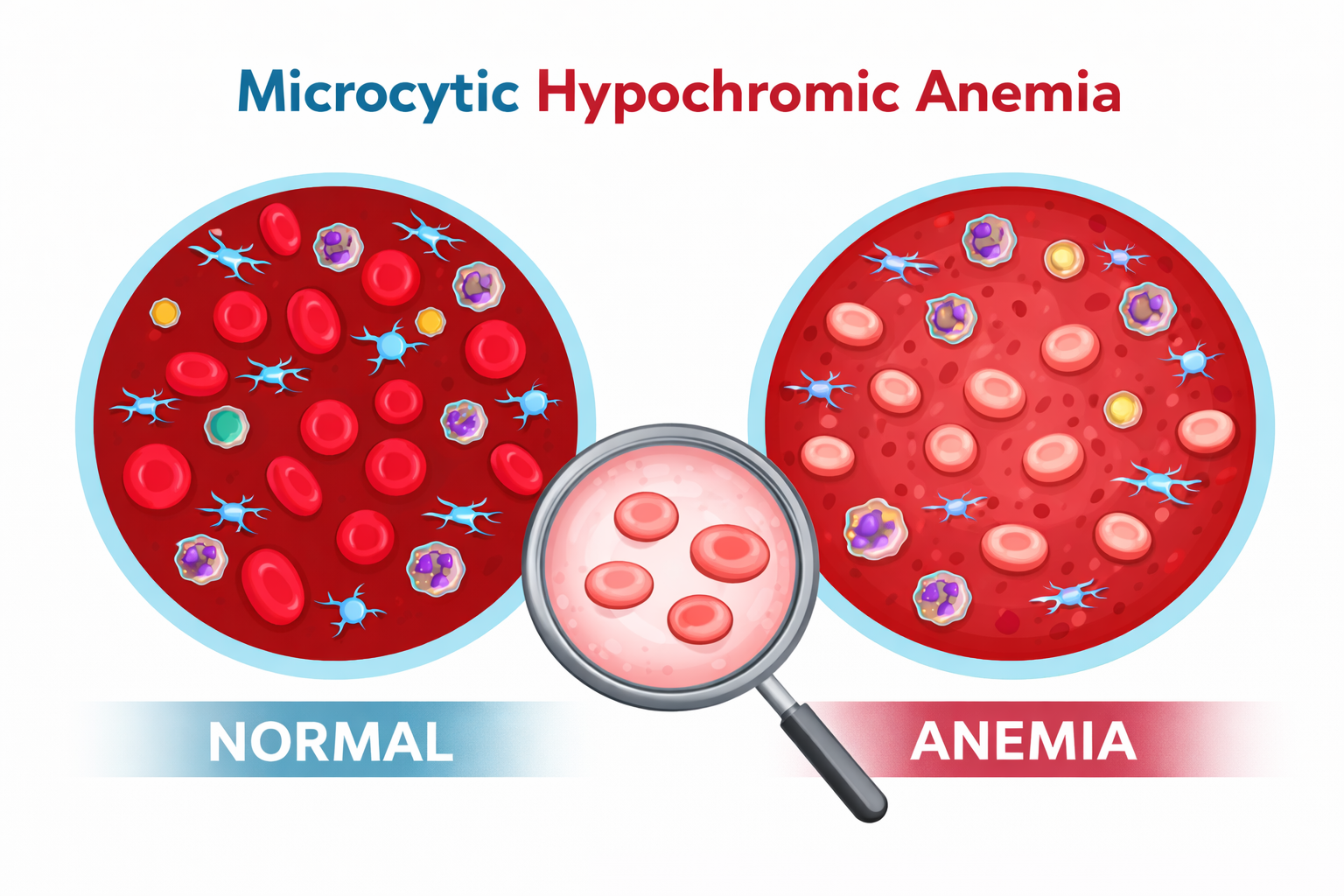
When iron stores fall, the bone marrow cannot produce enough hemoglobin. As a result, red blood cells become smaller and paler than normal.
This pattern is called microcytic hypochromic anemia — meaning small (microcytic) and pale (hypochromic) red cells.
Normal red blood cells compared with microcytic hypochromic red cells seen in iron deficiency anemia. The cells become smaller and contain less hemoglobin, making them appear pale.
Think of red blood cells as delivery trucks, and hemoglobin as the cargo hold inside each truck. When hemoglobin is low, each truck carries less oxygen per trip — and your organs and muscles begin to feel the shortage.
Iron deficiency progresses through three distinct stages:
Iron depletion — ferritin falls, but hemoglobin remains normal; no symptoms yet.
Iron-deficient red cell production — red cell production is affected, hemoglobin borderline; mild symptoms may appear.
Iron deficiency anemia — hemoglobin falls clearly below normal; symptoms become noticeable.
This is why ferritin is the most important early warning marker — it often falls months before hemoglobin drops.
Causes of Iron Deficiency Anemia
Three main mechanisms lead to iron deficiency:
1. Inadequate iron intake
A diet consistently low in iron-rich foods is a common contributor, particularly in vegetarian populations.
Plant-based (non-heme) iron is less efficiently absorbed than animal-based (heme) iron.
Therefore, vegetarians need to be more deliberate about meeting daily iron requirements.
2. Poor absorption
Even with an adequate diet, certain conditions reduce the gut’s ability to absorb iron.
For example, celiac disease, Helicobacter pylori (H. pylori) infection, inflammatory bowel disease, and long-term antacid use all impair absorption- either by damaging the intestinal lining or altering the gut environment.
3. Chronic blood loss
This is the most clinically important cause. Sources include:
Heavy or prolonged menstrual periods (menorrhagia)
Gastrointestinal bleeding from peptic ulcers, polyps, hemorrhoids, or colorectal cancer
Frequent blood donation
Urinary tract bleeding (less common)
Why Is It More Common in Women — And Why Do Men Need Extra Attention?
Why are women more commonly affected:
Women of reproductive age lose blood every month through menstruation — and with it, a significant amount of iron.
A heavy or prolonged period can deplete iron stores faster than diet alone can replenish them.
During pregnancy, iron demand increases even further, as the growing baby draws heavily on the mother’s iron reserves.
These are physiological (normal bodily) reasons, which is why iron deficiency is far more prevalent in women during these life stages.
Why men and post-menopausal women always need investigation:
Men do not have monthly blood loss. Post-menopausal women no longer menstruate. Therefore, neither group has a routine physiological reason to lose iron.
When iron deficiency anemia is found in these groups, it almost always points to a pathological cause — meaning something is wrong that needs to be identified.
The most important concern is gastrointestinal blood loss — from a peptic ulcer, gut polyp, or in some cases, colorectal cancer. This bleeding can be slow and completely silent — no visible blood in the stool — yet enough to steadily deplete iron stores over months.
Consequently, doctors take iron deficiency anemia in men and post-menopausal women seriously and typically investigate with a stool occult blood test or endoscopy, even when the patient feels relatively well.
In short, in women of reproductive age, the cause is usually clear. In men and post-menopausal women, iron deficiency anemia is a red flag that always warrants further investigation.
Symptoms of Iron Deficiency Anemia
Because iron deficiency develops gradually, many people adapt to its symptoms and mistake them for ordinary tiredness. However, the following signs together are clinically meaningful:
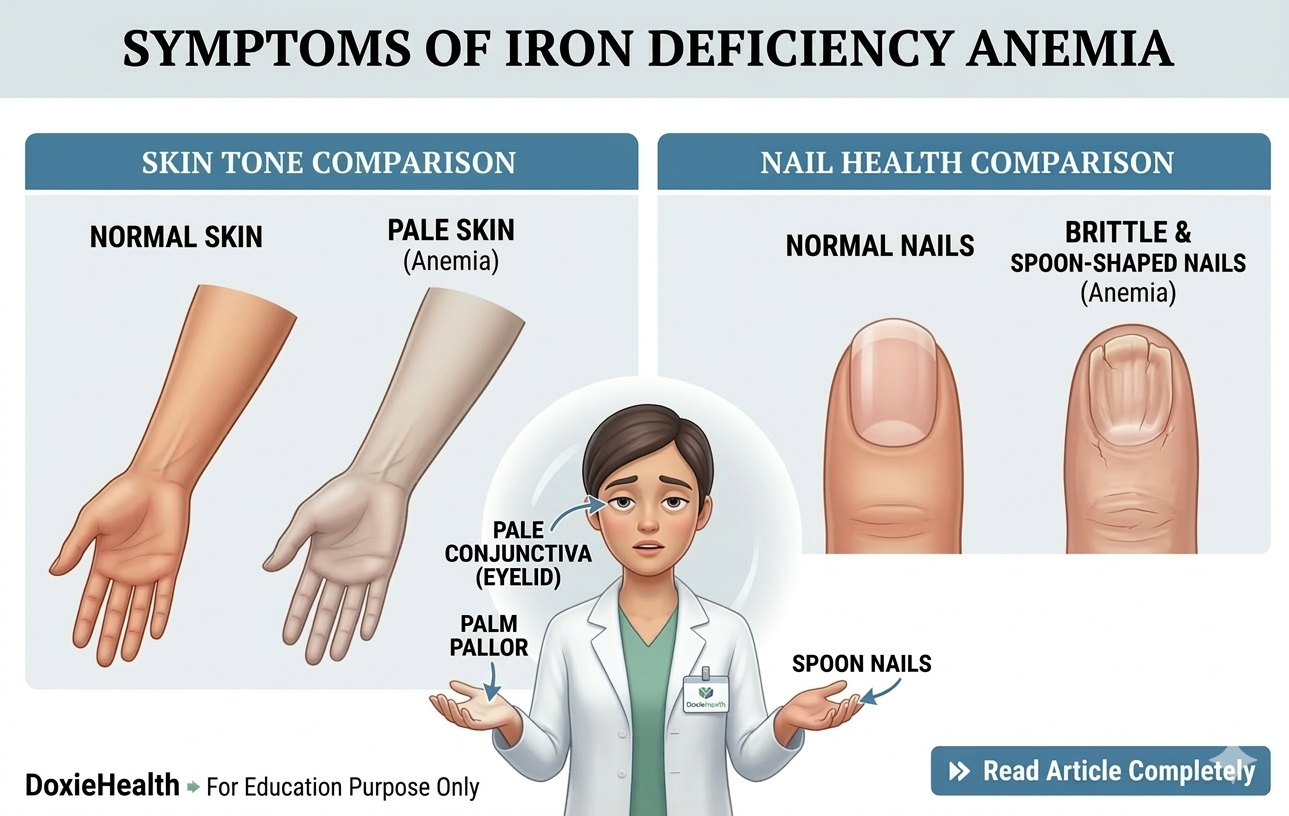
Common visible symptoms of iron deficiency anemia. Image: DoxieHealth
Persistent fatigue — the most common symptom; results directly from reduced oxygen delivery to tissues.
Pale skin and pale inner eyelids — a visible sign of low hemoglobin.
Shortness of breath on mild exertion, such as climbing stairs.
Dizziness or light-headedness
Frequent headaches
Cold hands and feet — from reduced circulation due to lower red cell mass.
Brittle or spoon-shaped nails (koilonychia) — a specific sign of chronic iron deficiency.
Hair thinning or increased hair fall — iron is essential for hair follicle function.
Pica — unusual cravings for non-food items such as ice, clay, or dirt; this lesser-known symptom is specific to iron deficiency.
One important nuance: Symptoms do not always reflect the severity of the numbers. Some people with significantly low hemoglobin feel relatively fine because the deficiency developed slowly.
Others feel severely symptomatic with only a mild drop. As a result, a blood test is always necessary — symptoms alone are not a reliable measure.
How Is Iron Deficiency Anemia Diagnosed?
Diagnosis involves a combination of blood tests. Your doctor will typically start with a Complete Blood Count (CBC) and then add specific iron studies to confirm the diagnosis. For a detailed explanation of how to read your CBC report, see our CBC Blood Test Explained guide on DoxieHealth.
CBC (Complete Blood Count) — checks hemoglobin, MCV, MCH, and RDW; shows the characteristic pattern of small, pale red cells.
Serum Ferritin — the most sensitive early marker; reflects your body’s iron stores; the first value to fall, even before hemoglobin drops.
Serum Iron — measures iron circulating in your blood; low in iron deficiency.
TIBC (Total Iron Binding Capacity) — measures how much iron your blood can carry; it rises when the body is starved of iron, as it tries harder to capture more.
Peripheral Blood Smear — allows the doctor to visually examine red cell size and colour under a microscope.
Stool Occult Blood Test — screens for hidden, invisible bleeding in the gut.
Blood Test Marker
Finding
Clinical Significance
Hemoglobin (Hb)
Low
Confirms anemia
MCV
Low
Red cells are smaller than normal
MCH
Low
Red cells carry less hemoglobin — appear pale
RDW
High
Mix of old normal and new small cells
Serum Ferritin
Low
First marker to fall; reflects iron stores
Serum Iron
Low
Circulating iron is reduced
TIBC
High
Body increases binding capacity when iron-starved
Key Insight: Ferritin below 30 µg/L is considered depleted even when hemoglobin is still normal — this is the iron depletion stage. Addressing it early prevents progression to full anemia. Therefore, always ask your doctor to check ferritin alongside your CBC if iron deficiency is suspected.
Severity of Iron Deficiency Anemia
Doctors classify iron deficiency anemia into three stages based on hemoglobin levels. This classification guides how urgently treatment is needed:
Severity
Hemoglobin in Women
Hemoglobin in Men
What It Means
Mild
10.0–11.9 g/dL
10.0–12.9 g/dL
Subtle symptoms; dietary changes and supplements are usually sufficient
Moderate
7.0–9.9 g/dL
7.0–9.9 g/dL
Noticeable symptoms: oral iron supplements required; the cause should be investigated
Severe
Below 7.0 g/dL
Below 7.0 g/dL
Significant symptoms; may require IV iron or blood transfusion; urgent evaluation needed
Based on the WHO classification of anemia severity.
Important These are general thresholds. Your doctor will always interpret your hemoglobin in the context of your symptoms, age, and overall health — not by numbers alone.
Treatment Overview
Treatment involves two equally important steps: replenishing iron and identifying the underlying cause.
Oral iron supplements — most commonly ferrous sulphate — are the standard first-line treatment and are effective for most people.
Dietary adjustments support recovery and help prevent recurrence.
For a full guide on iron-rich foods, supplement strategies, and practical lifestyle tips, see our upcoming article: Iron Deficiency Anemia: Prevention & Treatment (coming soon — Preventive Health).
However, supplements alone are not enough if the underlying cause is not addressed. A gut ulcer, untreated heavy periods, or poor absorption will cause deficiency to return even after successful treatment.
In severe cases, intravenous iron or blood transfusion may be required.
Key Clinical Insights
Ferritin is the most sensitive early marker – it falls long before hemoglobin drops. Always check it alongside your CBC if iron deficiency is suspected.
Tea and coffee reduce iron absorption when consumed with meals — a commonly overlooked fact, particularly relevant where chai is a daily habit.
Calcium competes with iron for absorption – therefore, iron supplements and calcium-rich foods or supplements should be taken at separate times.
H. pylori is an underrecognised cause of iron deficiency anemia that does not improve with supplements alone – testing is recommended when patients do not respond to treatment as expected.
Celiac disease should be considered in unexplained iron deficiency anemia, even without obvious digestive symptoms – it is one of the more commonly missed underlying causes.
👩⚕️ Doctor’s Note Iron deficiency anemia is common, treatable, and in most cases completely reversible. However, it always has a cause, and finding that cause is just as important as treating the deficiency itself.
Never start iron supplements without a confirmed blood test, and never assume fatigue alone means you are iron-deficient. Too much iron has its own risks.
Let your results guide the conversation with your doctor.
When Should You Be Concerned?
Speak to your doctor promptly if you notice any of the following:
Hemoglobin below 10 g/dL — significant anemia that requires prompt medical attention.
Ferritin below 12–30 µg/L — confirms depleted iron stores even if hemoglobin appears borderline.
Fatigue, breathlessness, and dizziness together — this combination always warrants a blood test.
Heavy periods soaking through pads quickly or lasting more than 7 days.
Black, tarry, or bloody stools — these require urgent evaluation without delay.
Anemia in a man or post-menopausal woman — always investigate for an underlying cause.
No improvement after 4–8 weeks of iron supplements — reassessment and further investigation are needed.
The Takeaway
Iron deficiency anemia is one of the most common and most treatable conditions your blood test can reveal.
Understanding what your results mean — and why they matter — puts you in a much stronger position when you walk into your doctor’s appointment.
The goal is not to self-diagnose, but to ask the right questions and make informed decisions about your health.
Questions to Ask Your Doctor
“Is my ferritin low, even if my hemoglobin looks normal?” — Ferritin depletion needs treatment too, not just monitoring.
“Do we need to investigate the cause, or just start supplements?” — especially important for men and post-menopausal women.
“Which iron supplement do you recommend and when should I take it?” — Timing and formulation significantly affect absorption.
“Should I avoid tea, coffee, or calcium around my supplement?” — The answer is yes, but your doctor can guide the timing.
“When should I recheck my blood test after starting treatment?” — typically 4–8 weeks after starting supplements.
“Do I need a stool test or endoscopy to rule out gut bleeding?” — particularly if the cause is not immediately obvious.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice



 Explained")
Leave a Reply