Iron deficiency anemia is entirely preventable in most people — and when it does develop, it is one of the most treatable nutritional conditions.
Whether you are at risk and want to stay ahead of it, or you have already been diagnosed and want to know what comes next, this guide covers both equally.
We walk through dietary prevention, smart supplementation, what to avoid, and how to monitor your recovery through blood tests.
Part 1: Prevention of Iron Deficiency Anemia— Keeping Iron Levels Healthy
Prevention is most relevant for those at higher risk — women of reproductive age, vegetarians, pregnant women, and anyone with a history of iron deficiency.
The goal is to maintain iron stores at a healthy level before anemia develops. The first sign of trouble is a falling ferritin — often months before hemoglobin drops.
Who Should Focus on Prevention of Iron Deficiency Anemia?
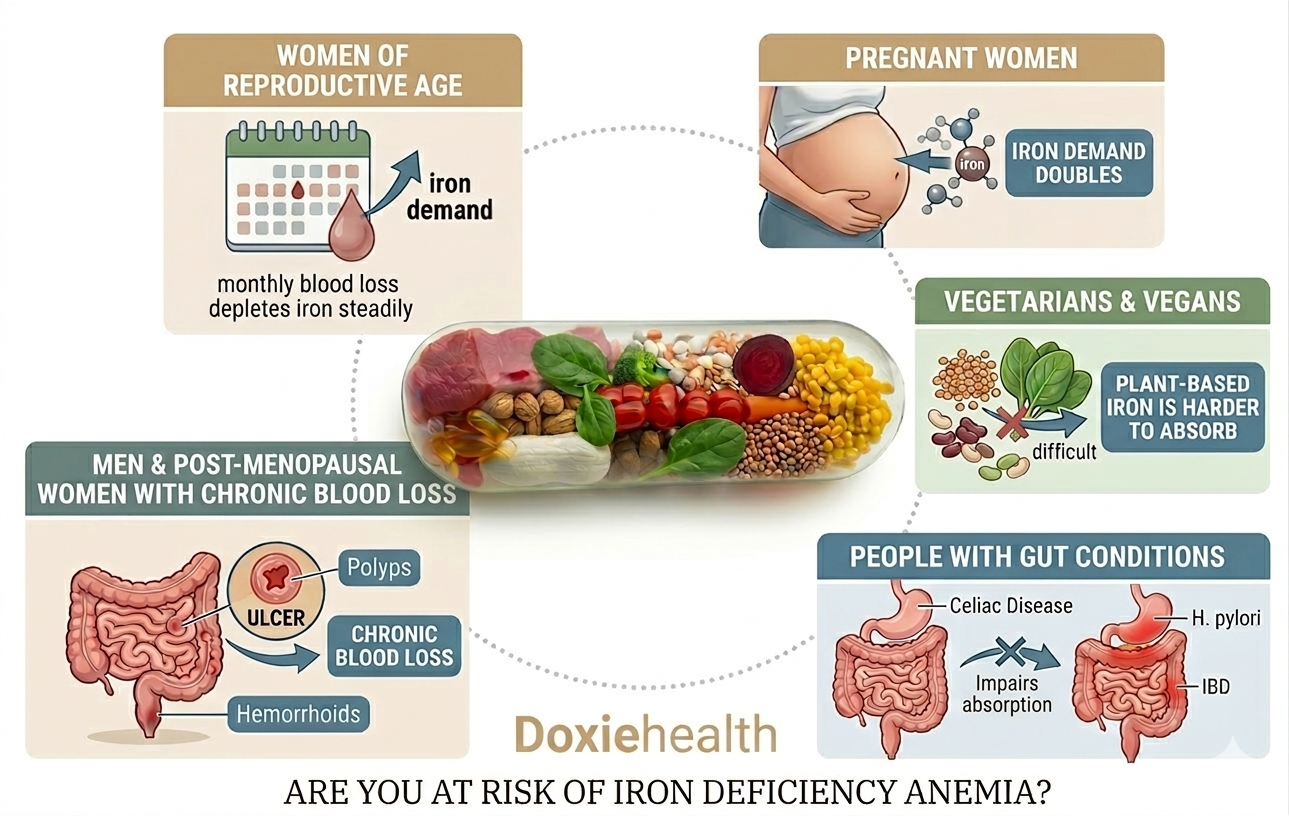
Who is most at risk of iron deficiency anemia. Image: DoxieHealth
Women of reproductive age — monthly blood loss depletes iron steadily
Pregnant women — iron demand doubles during pregnancy
Vegetarians and vegans — plant-based iron is harder to absorb
People with gut conditions — celiac disease, IBD, or H. pylori impair absorption
Men and post-menopausal women with chronic blood loss from gut ulcers, polyps, or hemorrhoids
Preventive & Management Diet for Iron Deficiency Anemia— Eat These Foods Regularly
Getting enough iron from food is the foundation of prevention. There are two types of dietary iron, and your body absorbs them very differently:
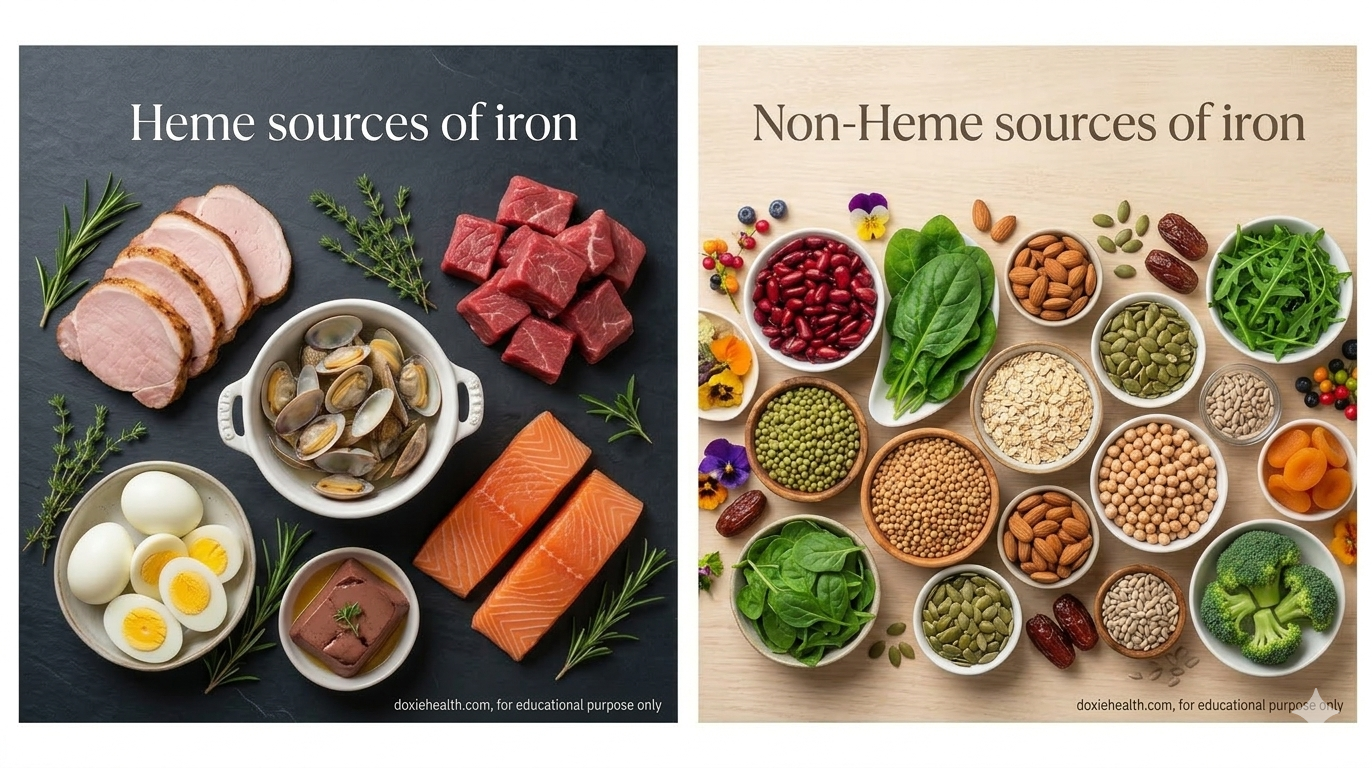
Heme and non-heme iron food sources for iron deficiency anemia. Image: DoxieHealth
Heme iron (animal sources) — absorbed at 15–35% efficiency. The most bioavailable form.
Non-heme iron (plant sources) — absorbed at only 2–20% efficiency. Can be improved significantly with the right food combinations.
Food
Iron per 100g
Type
Chicken or lamb liver
6–9 mg
Heme
Red meat (beef, lamb)
2–4 mg
Heme
Oysters
5–7 mg
Heme
Eggs (whole)
1.2 mg
Heme (moderate)
Pumpkin seeds
8.8 mg
Non-heme
Lentils (cooked)
3.3 mg
Non-heme
Spinach (cooked)
3.6 mg
Non-heme
Tofu
2.7 mg
Non-heme
Kidney beans
2.9 mg
Non-heme
Fortified cereals
4–8 mg
Non-heme
Dark chocolate (70%+)
3.3 mg
Non-heme
Reference: USDA FoodData Central
Note on eggs: Eggs contain a moderate amount of heme iron. However, they also contain phosvitin — a protein that can inhibit iron absorption. Eating eggs alongside other iron-rich foods may slightly reduce overall absorption. Eggs are still a useful iron source, but not the most efficient one.
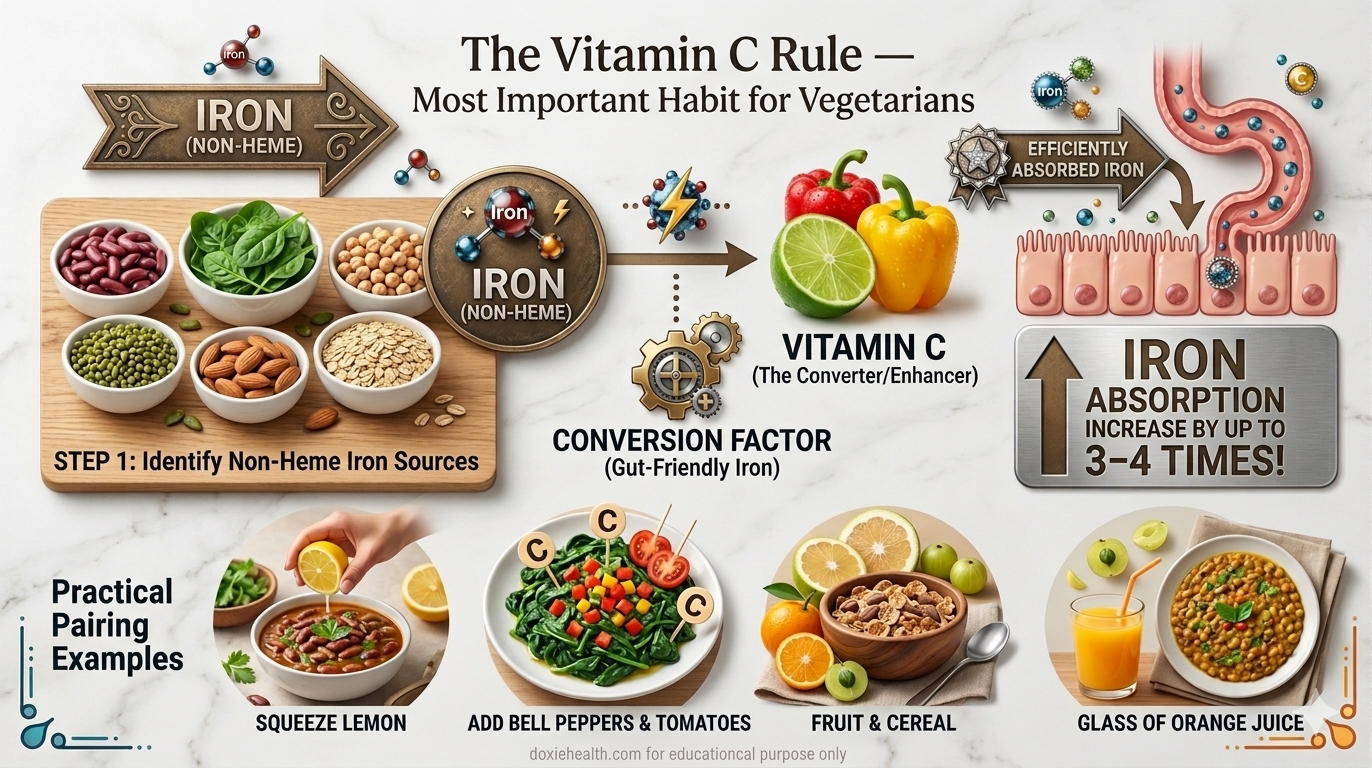
The Vitamin C Rule — Most Important Habit for Vegetarians
Pairing iron-rich foods with Vitamin C significantly boosts iron absorption. Image: DoxieHealth
Vitamin C converts non-heme iron into a form that the gut absorbs far more efficiently.
Pairing plant-based iron with Vitamin C at the same meal can increase absorption by up to 3–4 times.
Practical examples:
Squeeze lemon juice over dal, lentil soup, or rajma
Add tomatoes or bell peppers to spinach dishes
Eat citrus fruit or amla alongside fortified cereal
Drink a small glass of orange juice with your iron-rich meal
What to Avoid — Foods and Habits That Block Iron
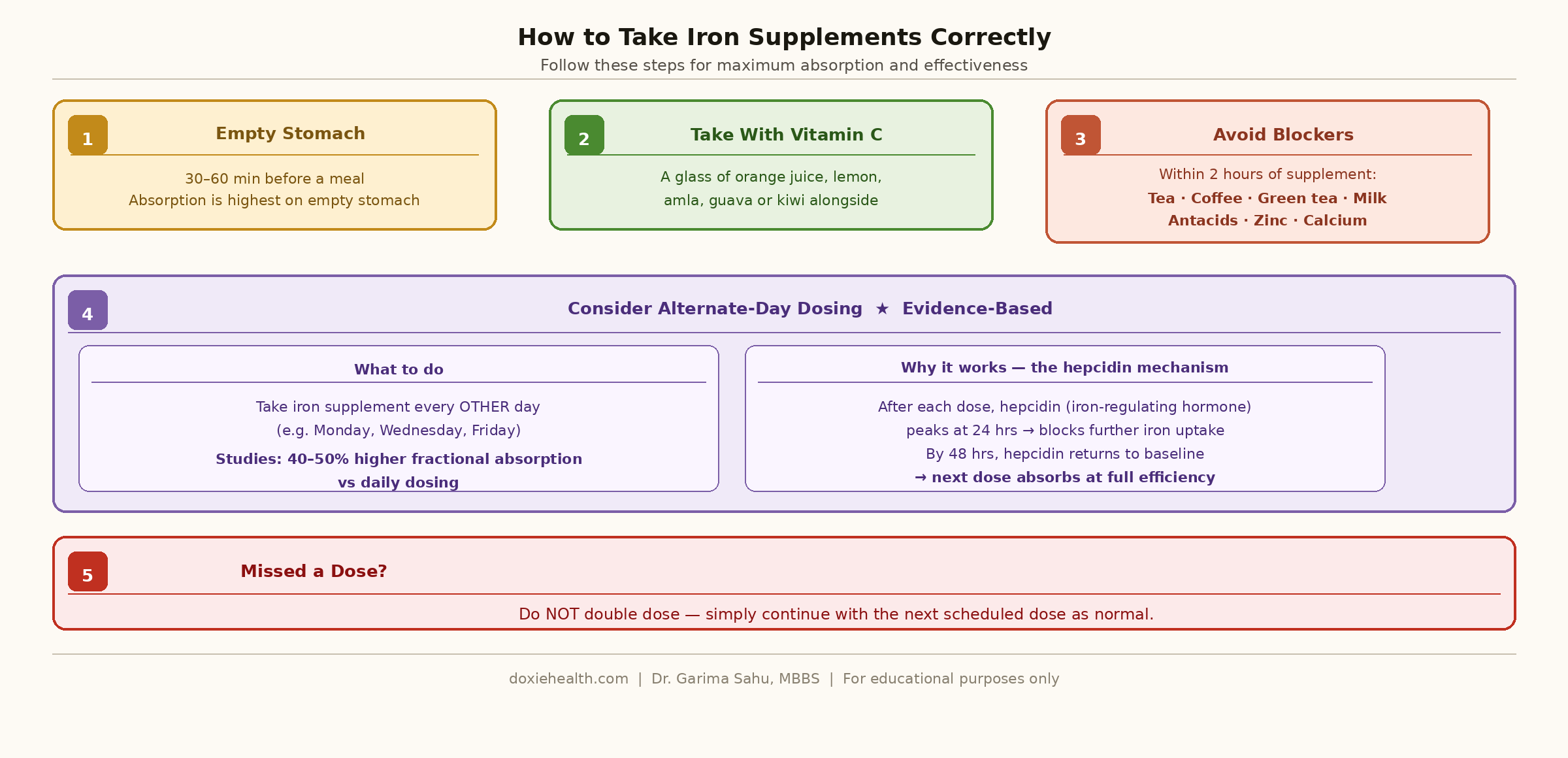
How to take iron supplements for maximum absorption. Diagram: DoxieHealth
Several common habits significantly reduce iron absorption. These apply whether you are preventing iron deficiency or recovering from it.
Tea and coffee — tannins bind iron and block absorption. Avoid within 1 hour before or after iron-rich meals or supplements. Highly relevant where chai is consumed throughout the day.
Green tea — contains even higher levels of tannins than regular tea, making it particularly potent at blocking iron absorption. Do not consume green tea around iron-rich meals or supplement doses.
Calcium-rich foods — milk, yogurt, cheese, and calcium supplements compete with iron for absorption. Take iron supplements and calcium at least 2 hours apart.
Zinc supplements — iron and zinc compete for the same intestinal absorption pathway (DMT1). Taking them together reduces the effectiveness of both. If you need both, take them at least 2 hours apart.
Phytates — found in whole grains and legumes. Soaking, sprouting, or fermenting these foods before cooking reduces phytate content and improves iron absorption.
Antacids and PPIs — reduce stomach acid needed for iron absorption. If you take these regularly, ask your doctor to monitor your iron levels.
Preventive Testing for Iron Deficiency Anemia — When to Check Your Iron
Getting your ferritin checked regularly is the most reliable way to catch iron depletion early — before it becomes anemia.
Group
Recommended Testing
What to Check
Women of reproductive age
Once a year
CBC + Ferritin
Pregnant women
First trimester + 28 weeks
CBC + Ferritin + Iron studies
Vegetarians / vegans
Every 6–12 months
Ferritin
People with heavy periods
Every 6 months
CBC + Ferritin
People with gut conditions
Every 6–12 months
CBC + Ferritin + Iron studies
General adults (low risk)
Every 2–3 years
CBC
For a full explanation of what ferritin, serum iron, and TIBC mean on your blood test, see our Iron Studies Explained guide on DoxieHealth.
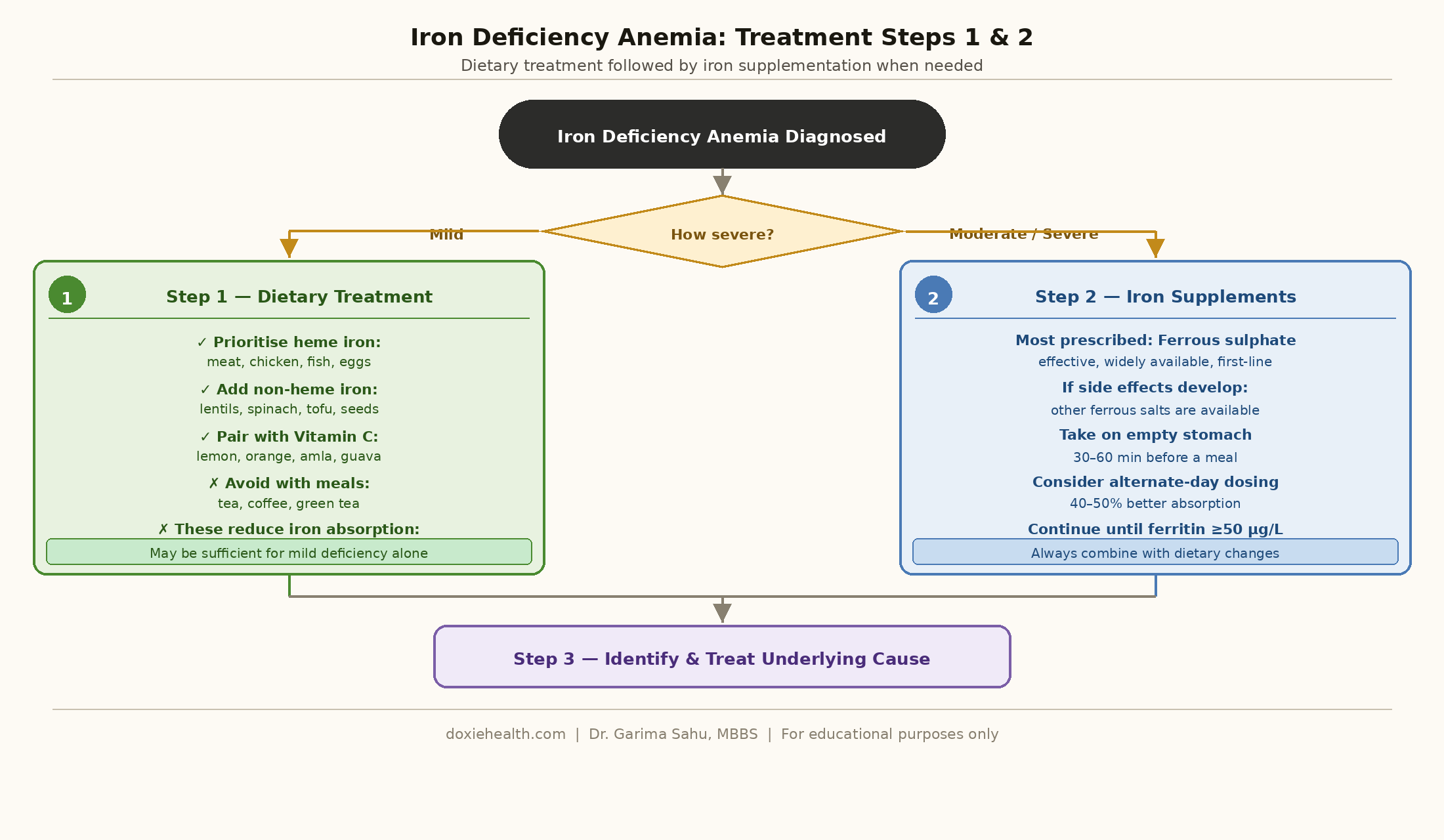
Part 2: Treatment — What to Do When Iron Deficiency Anemia Is Diagnosed
Treatment for iron-deficiency anemia has two equally important goals:
Replenishing iron stores and restoring hemoglobin
Identifying the underlying cause
Treating the deficiency without finding the cause means it will return. Your doctor will always try to establish why iron levels fell, even as treatment begins.
Treatment steps for iron deficiency anemia — diet and iron supplements. Diagram: DoxieHealth
Step 1 — Treat With Diet
For mild deficiency, dietary changes alone may be sufficient.
Even for moderate to severe deficiency, improving diet supports supplement treatment and helps prevent recurrence.
Follow the same dietary guidelines outlined in Part 1 — prioritize heme iron sources, pair plant-based iron with Vitamin C, and eliminate absorption blockers.
Step 2 — Iron Supplements
For moderate to severe deficiency, dietary changes alone are insufficient. Iron supplements are the standard treatment and are highly effective when taken correctly.
Type
Absorption
Tolerability
Notes
Ferrous sulphate
High
Moderate side effects
Most prescribed, cheapest, first-line
Ferrous fumarate
High
Moderate
Slightly better tolerated than sulphate
Ferrous gluconate
Moderate
Better tolerated
Good option if sulphate causes nausea
Ferric iron (Fe³⁺)
Moderate
Fewer side effects
Often better for sensitive stomachs
IV iron (infusion)
Direct (bypasses gut)
Rare reactions
For severe cases or malabsorption
How to Take Iron Supplements Correctly
Take on an empty stomach — 30–60 minutes before a meal for best absorption
Take with Vitamin C — a glass of orange juice increases absorption significantly
Avoid tea, coffee, green tea, milk, antacids, zinc, and calcium within 2 hours of taking your supplement
Consider alternate-day dosing — clinical studies show that taking iron every other day results in 40–50% higher fractional iron absorption compared to daily dosing.
This works because serum hepcidin (the hormone that controls iron uptake) peaks at 24 hours after a dose and returns to baseline by 48 hours — allowing better absorption on the next dose day.
Do not double-dose if you miss one — continue with the next scheduled dose
Managing Side Effects
Iron supplements commonly cause gastrointestinal side effects. These are normal and manageable:
Constipation — increase water intake and dietary fibre. Switch formulation if severe.
Black or dark stools — completely normal. Not a cause for concern.
Nausea — take with a small amount of food, or switch to ferrous gluconate.
Stomach cramps — switch from ferrous sulphate to a gentler formulation.
If side effects prevent you from taking supplements consistently, speak to your doctor about switching to an IV iron infusion.
Step 3 — IV Iron (When Oral Is Not Enough)
In some situations, oral supplements are not sufficient. IV iron delivers iron directly into the bloodstream, bypassing the gut entirely.
IV iron is used when:
Oral iron is not tolerated due to severe side effects
A gut condition, such as celiac disease or IBD, prevents absorption
Hemoglobin is critically low and needs rapid correction
Iron deficiency keeps recurring despite adequate oral treatment
IV iron is given as a clinic infusion, typically over 15–60 minutes. Most people see significant improvement in hemoglobin within 2–4 weeks.
Step 4 — Treat the Underlying Cause
Supplements replenish iron — but they do not fix the reason iron fell. Treating the root cause is essential to prevent recurrence.
Underlying Cause
Management
Heavy periods (menorrhagia)
Gynecologist referral — hormonal therapy, IUD, or investigation for fibroids
Gut bleeding (ulcer, polyp)
Endoscopy or colonoscopy to identify and treat the source
H. pylori infection
Antibiotic eradication course — resolves both absorption impairment and gut bleeding
Celiac disease
Strict gluten-free diet — restores gut absorption over time
Poor dietary intake
Dietitian referral for a sustainable iron-rich eating plan
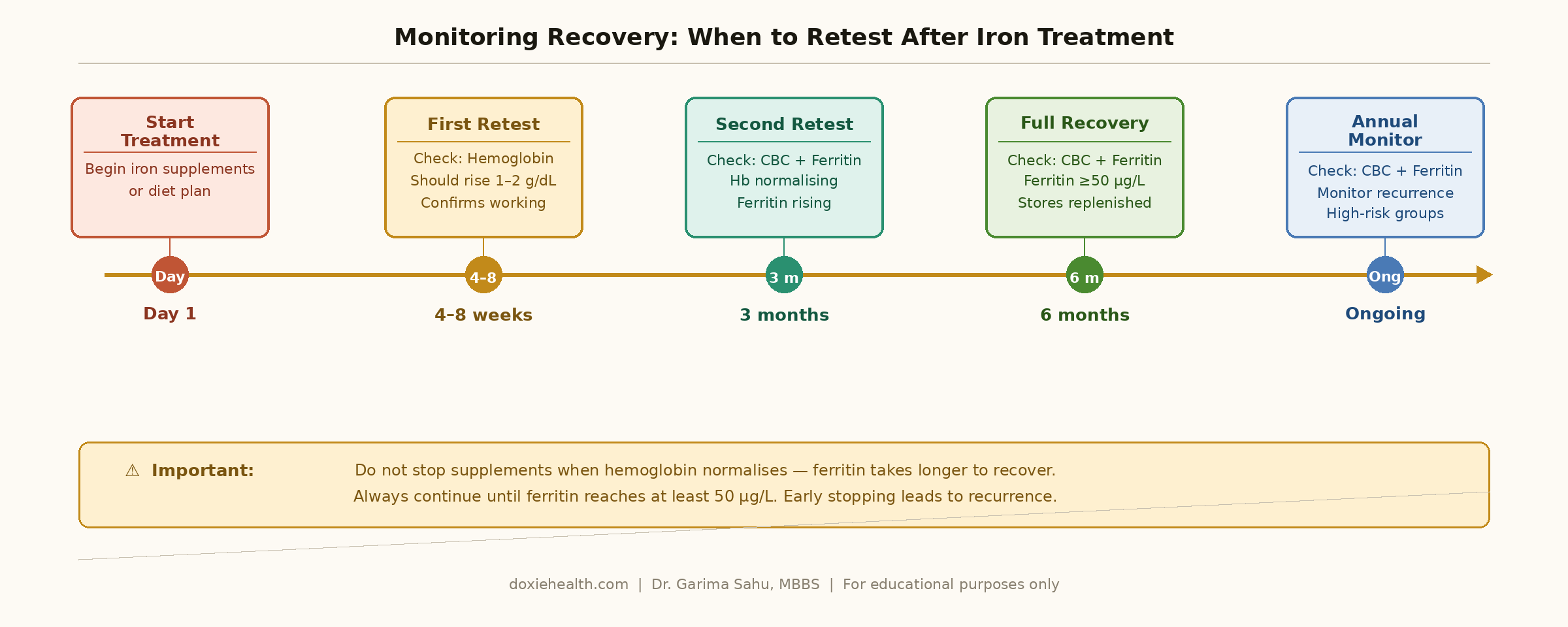
Part 3: Monitoring Recovery From Iron Deficiency Anemia — When to Retest
Regular blood testing is essential to confirm treatment is working and to know when it is safe to stop.
The most common mistake is stopping supplements too early — when hemoglobin normalises but ferritin is still depleted.
When to retest your blood after starting iron deficiency anemia treatment. Diagram: DoxieHealth
Timepoint
Test
What to Look For
4–8 weeks after starting
Hemoglobin
Should rise by 1–2 g/dL — confirms supplements are working
3 months after starting
CBC + Ferritin
Confirm stores are fully restored before stopping supplements
6 months after starting
CBC + Ferritin
Ferritin should reach at least 50 µg/L — stores replenished
After completing treatment
Ferritin
Confirm stores fully restored before stopping supplements
Annually (ongoing)
CBC + Ferritin
Monitor for recurrence in high-risk groups
⚠️ Important: Do not stop supplements when hemoglobin normalizes — ferritin takes longer to recover. Always continue until ferritin reaches at least 50 µg/L. Stopping early is the most common reason iron deficiency anemia returns.
Key Clinical Insights
Iron and zinc must not be taken together — they compete for the same intestinal absorption pathway (DMT1). Studies show iron supplementation alone has higher cure rates than iron combined with zinc. If both are needed, take them at least 2 hours apart.
Alternate-day iron dosing results in 40–50% higher fractional iron absorption compared to daily dosing — because hepcidin peaks at 24 hours after a dose and returns to baseline by 48 hours, allowing better uptake on the next dose day.
Hemoglobin recovers faster than ferritin — continue supplements until ferritin reaches at least 50 µg/L, not just until hemoglobin normalizes.
H. pylori eradication should be considered in patients who do not respond to iron supplements — it is one of the most commonly missed reasons for treatment failure.
Vitamin C supplementation (500 mg) taken alongside iron can significantly improve absorption — particularly for non-heme iron sources.
Never self-supplement long-term without monitoring — iron overload is a real risk if supplements are taken without blood test confirmation.
👩⚕️ Doctor’s Note Iron deficiency anemia is highly treatable — but treatment requires patience. Hemoglobin starts improving within 4 weeks, but fully replenishing iron stores takes 3–6 months of consistent supplementation. Do not stop early just because you feel better. Always address the underlying cause alongside supplementation — otherwise, the deficiency will return. Your blood test results are your most reliable guide throughout this process.
When Should You Be Concerned?
Speak to your doctor promptly if:
Hemoglobin has not improved after 4–8 weeks of iron supplements — reassessment is needed
Side effects are severe enough to prevent consistent supplement use
Ferritin remains low despite completing a full course of treatment
Symptoms worsen — increasing breathlessness, chest pain, or severe fatigue
Iron deficiency recurs after completing treatment — always needs investigation
The Takeaway
Iron deficiency anemia is preventable in most people — and when it does develop, it is fully reversible with the right approach.
Prevention means eating iron-rich foods consistently, pairing them with Vitamin C, avoiding absorption blockers, and testing ferritin regularly if you are at risk.
Treatment means the right supplement, taken correctly, for long enough — and always addressing the underlying cause.
Questions to Ask Your Doctor
“Is my ferritin low even if my hemoglobin looks normal?” — depletion needs treatment before anemia develops
“Which iron supplement do you recommend, and how should I take it?” — formulation and timing matter significantly
“Can I take iron every other day instead of daily?” — Alternate-day dosing may improve absorption
“Should I avoid zinc supplements while taking iron?” — yes, take them at least 2 hours apart
“When should I retest my hemoglobin and ferritin?” — get a clear timeline before leaving the appointment
“When can I safely stop taking iron supplements?” — the answer depends on ferritin, not just hemoglobin
References & Further Reading
Kasper DL et al. Harrison’s Principles of Internal Medicine, 21st ed. McGraw-Hill, 2022.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice




 Explained")
Leave a Reply