If your doctor has ordered iron studies alongside your routine blood test, you may find yourself staring at unfamiliar terms — serum iron, ferritin, TIBC — without a clear understanding of what they actually mean in your iron test results.
Each of these markers tells a different part of the same story: how much iron your body has, how it is being transported, and whether your stores are running low.
In this guide, we explain each iron study marker in plain language, what normal and abnormal results mean, and what your doctor is looking for.
What Are Iron Studies?
Iron studies are a group of blood tests that together assess your body’s iron status more completely than a CBC alone.
While a Complete Blood Count can detect anaemia, it cannot always identify the cause.
Iron studies fill that gap — they reveal whether iron deficiency, iron overload, or another problem is the underlying cause of abnormal findings.
If you have not yet read our CBC Blood Test Explained guide on DoxieHealth, it provides important context for understanding how these markers connect to your overall blood count results.
CBC blood test results show low haemoglobin, low MCV, or high RDW — suggesting possible iron deficiency anaemia.
Experiencing symptoms such as persistent fatigue, hair loss, or breathlessness.
Pregnancy is planned or confirmed — iron demand increases significantly during this time
Iron deficiency treatment is underway — to track whether supplements are working
Iron overload is suspected — a condition where too much iron accumulates in organs
Quick Reference: Normal Iron Studies Ranges
General adult reference ranges. Your lab may show slightly different values.
Marker
Normal Range (Adults)
Unit
Serum Iron
60–170 (women) / 65–176 (men)
µg/dL
Serum Ferritin
12–150 (women) / 12–300 (men)
µg/L (ng/mL)
TIBC
240–450
µg/dL
Transferrin Saturation
20–50%
%
Serum Transferrin
200–360
mg/dL
Reference: Harrison’s Principles of Internal Medicine, 21st ed.
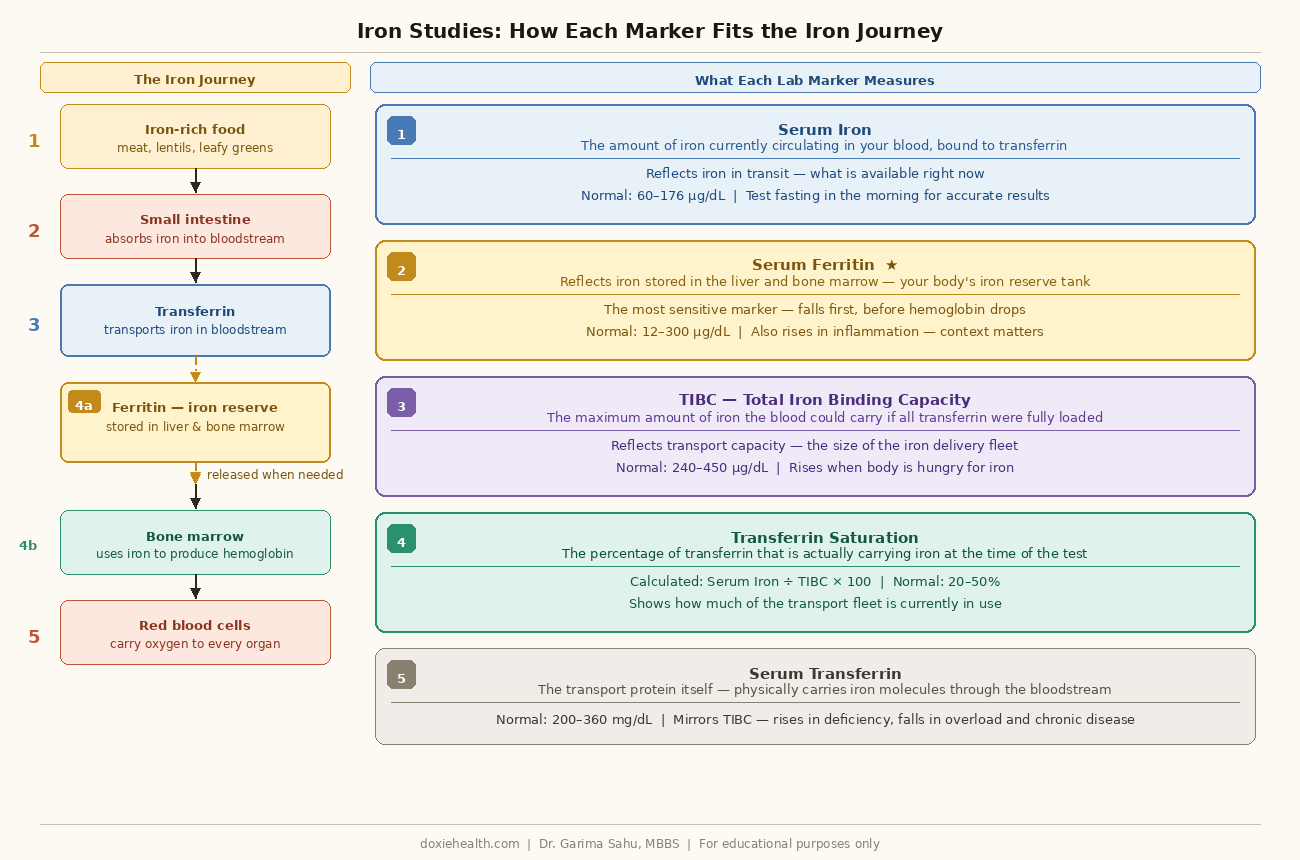
How iron travels through your body and what each iron study marker measures. Diagram: DoxieHealth
Serum Iron
Serum iron measures the amount of iron currently circulating in your bloodstream — specifically, the iron that is bound to transferrin and actively in transit.
It is essentially a snapshot of how much iron is available at the moment of testing and is one of the key components of your iron panel.
Low Serum Iron: What It Means
Low serum iron is the most recognisable finding in iron deficiency.
However, serum iron fluctuates significantly throughout the day, peaking in the morning and dropping in the evening.
It also drops temporarily during infection or inflammation, even when iron stores are adequate. Therefore, serum iron alone is never enough to confirm iron deficiency.
High Serum Iron: What It Means
Elevated serum iron can occur with:
Iron overload conditions, such as haemochromatosis — a genetic condition where the body absorbs too much iron
Recent iron supplement use or iron infusion
Liver disease- which can release stored iron into the blood
Repeated blood transfusions
Serum Ferritin
Ferritin is the storage protein for iron — it reflects how much iron your body has in reserve.
Think of serum ferritin as a fuel gauge: it shows you how full your iron tank is, not just what is currently in the engine.
Ferritin is the most clinically important marker in iron studies because it falls first – often months before haemoglobin drops. It also rises in iron overload, making it useful at both ends of the spectrum.
A low ferritin level often indicates depleted iron stores, even before anaemia develops.
Understanding high ferritin causes is equally important, as elevated levels may reflect inflammation, liver disease, or iron overload rather than excess iron alone.
Ferritin Level
Interpretation
Below 12 µg/L
Confirms iron deficiency — stores are depleted
12–30 µg/L
Low-normal — iron depletion likely, especially with symptoms
30–300 µg/L
Normal range
Above 300 µg/L (women) / 400 µg/L (men)
Elevated — investigate for iron overload or inflammation
One important nuance: Ferritin is also an acute phase reactant — meaning it rises during infection, inflammation, or liver disease, even when iron stores are genuinely low.
Therefore, a normal or high ferritin does not always rule out iron deficiency if inflammation is present. Your doctor will interpret ferritin alongside CRP or ESR to account for this.
For a detailed explanation of how low ferritin connects to iron deficiency anaemia, see our Iron Deficiency Anaemia guide on DoxieHealth.
TIBC measures the maximum amount of iron your blood could carry if transferrin were fully loaded.
It reflects how much capacity the blood has to bind and transport iron — essentially the size of the transport fleet, not just how many vehicles are currently in use.
This makes TIBC an important parameter when interpreting your iron test results, especially in suspected iron deficiency.
When iron stores are low, the body responds by producing more transferrin — increasing its capacity to capture every available iron molecule from the gut. As a result, TIBC rises in iron deficiency.
TIBC Level
Interpretation
High (above 450 µg/dL)
Suggests iron deficiency — body is hungry for iron
Normal
Suggests iron deficiency — the body is hungry for iron
Low (below 240 µg/dL)
Suggests iron overload, chronic disease, or malnutrition
Transferrin Saturation
Transferrin saturation tells you what percentage of transferrin is actually carrying iron at the time of the test.
It is one of the most useful values in an iron panel blood test because it combines information from both serum iron and TIBC.
A normal transferrin saturation is 20–50%. This means that under normal conditions, roughly one-third of your body’s iron transport capacity is being used.
Why does this matter clinically?
A low transferrin saturation (below 20%) alongside low ferritin strongly confirms iron deficiency anaemia.
A high transferrin saturation (above 50–60%) is a red flag for iron overload — particularly haemochromatosis, where excess iron deposits in the liver, heart, and joints.
Serum Transferrin
Transferrin is the protein that physically carries iron through the bloodstream — the transport vehicle itself.
When iron stores fall, the liver produces more transferrin to maximise iron capture. Therefore, transferrin levels mirror TIBC closely — both rise in deficiency and fall in overload or chronic disease.
Serum transferrin is less commonly ordered than the other markers. It is sometimes used to calculate transferrin saturation or to assess nutritional status, since transferrin production depends on adequate protein nutrition.
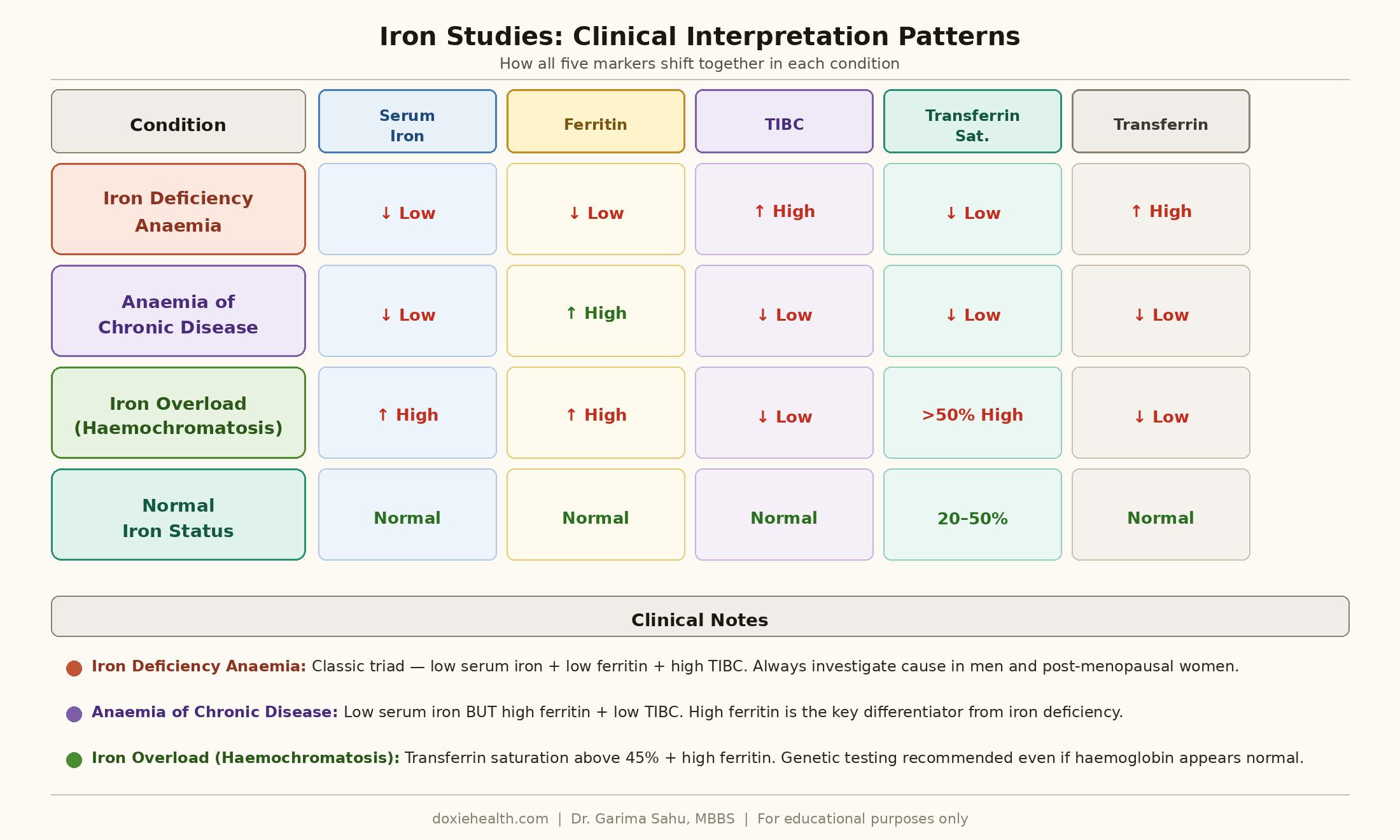
How Doctors Read Iron Studies Together
No single iron marker tells the complete story. Doctors always interpret these results as a pattern:
Iron studies clinical interpretation patterns iron deficiency anaemia chronic disease haemochromatosis
This pattern recognition is why your doctor orders the full Iron studies panel rather than a single test — each marker confirms or questions what the others are showing.
Key Clinical Insights
Ferritin below 30 µg/L warrants attention: Ferritin is considered the most sensitive marker for early iron deficiency in clinical practice.
Even when haemoglobin is still normal, this is the iron depletion stage, and treating it early prevents progression to full anaemia.
Inflammation artificially raises ferritin — a ferritin of 80 µg/L during an active infection may mask true iron deficiency. Your doctor may request a CRP to assess this.
Serum iron should always be drawn fasting in the morning — it drops significantly after meals and in the afternoon, which can lead to falsely low results.
Haemochromatosis is underdiagnosed — elevated transferrin saturation above 45% in a young adult, especially with fatigue and joint pain, should prompt genetic testing even if haemoglobin is normal.
Iron deficiency and anaemia of chronic disease can coexist in patients with inflammatory conditions like rheumatoid arthritis or IBD; careful interpretation of the full panel is needed.
👩⚕️ Doctor’s Note Iron studies are most useful when read as a complete panel — not as isolated numbers. A low serum iron alone means very little without ferritin and TIBC to give it context. Always bring your full report to your appointment, not just individual values. And if you are taking iron supplements, mention this to your doctor — it directly affects serum iron and transferrin saturation results.
When Should You Be Concerned?
Discuss your results with your doctor promptly if:
Ferritin below 12 µg/L — iron stores are depleted; treatment is needed
Ferritin 12–30 µg/L with symptoms — low-normal with fatigue or hair loss warrants treatment
Transferrin saturation above 50% — investigate for iron overload, particularly haemochromatosis
Low serum iron + high TIBC + low ferritin together — this classic triad confirms iron deficiency anaemia
Iron deficiency in a man or post-menopausal woman always requires investigation for a source of blood loss
The Takeaway
Iron studies give your doctor a complete picture of your body’s iron status — from circulating iron to stored reserves to transport capacity.
Understanding your iron test results and what each marker means helps you walk into your appointment informed and ask the right questions.
A single abnormal value rarely tells the whole story — the pattern across all markers is what matters.
Questions to Ask Your Doctor
“Is my ferritin low even if my haemoglobin looks normal?” — depletion needs treatment before anaemia develops
“Should I get iron studies done fasting and in the morning?” — timing significantly affects serum iron results
“Could my ferritin be falsely normal because of inflammation?” — important if you have a chronic condition
“My transferrin saturation is high — should I be tested for haemochromatosis?” — worth asking if above 45%
“How often should I recheck iron studies after starting supplements?” — typically every 4–8 weeks
References & Further Reading
Kasper DL et al. Harrison’s Principles of Internal Medicine, 21st ed. McGraw-Hill, 2022.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice



 Explained")
Leave a Reply