You received a LFT (liver function test) report — and now you are staring at values like SGPT, ALP, and bilirubin with no idea what they mean. That is exactly why this article exists. Here, we walk you through every liver function test result in plain language, so you can understand not just the number, but the story behind it.
Your liver is one of the hardest-working organs in your body. It filters toxins from your blood, produces bile for digestion, manufactures essential proteins, stores energy, and processes almost everything you eat, drink, or swallow -including medications. Here is a quick look at its most important roles.
Image: DoxieHealth | What your liver does — every single day
What Is a Liver Function Test (LFT)?
An LFT is not a single test — it is a panel of blood tests that together assess how well your liver is functioning. Doctors order it to screen for liver disease, monitor existing conditions, or assess how long-term medications affect the liver over time.
Normal LFT Reference Ranges at a Glance
Reference ranges can vary slightly between laboratories. Always compare your results against your own lab’s reference interval printed on your report.
Parameter
Normal Range
Units
Alkaline Phosphatase (ALP)
45 – 129
U/L
Bilirubin – Total
0.3 – 1.2
mg/dL
Bilirubin – Direct
0 – 0.20
mg/dL
Bilirubin – Indirect
0 – 0.9
mg/dL
GGT
< 55
U/L
SGOT (AST)
< 35
U/L
SGPT (ALT)
< 45
U/L
SGOT / SGPT Ratio
< 2
Ratio
Total Protein
5.7 – 8.2
g/dL
Albumin
3.2 – 4.8
g/dL
Globulin
2.5 – 3.4
g/dL
A/G Ratio
0.9 – 2
Ratio
Understanding Your LFT Results
Your LFT parameters are grouped into three categories — each telling a different part of the liver’s story:
Bilirubin values — how well the liver is processing and clearing waste
Liver enzymes (ALP, GGT, SGOT, SGPT) — whether liver cells are damaged or bile flow is blocked
Proteins (Albumin, Globulin, Total Protein) — how well the liver is manufacturing essential substances
Let’s go through each one.
Bilirubin — The Waste Disposal Story
Every day, your body breaks down old red blood cells that have reached the end of their lifespan. When these cells break down, they release a yellow pigment called bilirubin.
This bilirubin — still unprocessed at this stage — travels through the bloodstream to the liver. The liver then chemically processes it (a step called conjugation), making it water-soluble so it can be safely removed from the body.
Once processed, the bilirubin is passed into bile, a digestive fluid produced by the liver and stored in the gallbladder. Bile carries this waste into the intestine, from where it is eventually excreted.
🟡 What is bile? Bile is a yellow-green fluid made by the liver. It has two jobs: breaking down fats in food during digestion and acting as the liver’s waste-disposal route – carrying bilirubin and other byproducts out of the body. When bile flow is blocked, bilirubin builds up in the blood — and that is when you see jaundice.
This entire journey — from red cell breakdown to excretion — is what the three bilirubin values on your report are measuring.
Total Bilirubin
Total bilirubin is the combined level of all bilirubin in your blood. Think of it as the overall traffic on the waste clearance highway.
When it rises, it means either too much waste is being produced or the clearance route is blocked somewhere.
Indirect (Unconjugated) Bilirubin
Indirect bilirubin is the unprocessed form — bilirubin that has left the red cells but has not yet been handled by the liver.
A raised indirect bilirubin means either:
The liver cannot keep up with processing (liver dysfunction), or
Too many red blood cells are breaking down at once (as in haemolytic anaemia)
Direct (Conjugated) Bilirubin
Direct bilirubin is the processed form — already handled by the liver and ready to leave the body through bile. When this is raised, it usually means the exit route is blocked.
Common causes include gallstones, bile duct obstruction, or liver inflammation, preventing bile from draining normally.
When bilirubin accumulates significantly in the blood, it deposits in the skin and eyes — producing the yellow discolouration known as jaundice.
Liver Enzymes — The Damage Detectors
Think of liver enzymes as workers stationed inside your liver cells. Under normal conditions, they carry out their tasks quietly and stay inside the cells.
But when liver cells are damaged, inflamed, or under stress, these enzymes leak into the bloodstream — and that is what shows up as a raised value on your report.
Each enzyme leaks under slightly different circumstances, which is why doctors read them together rather than in isolation.
ALP — Alkaline Phosphatase
What it does: ALP is found mainly in the cells lining the bile ducts inside the liver, as well as in bone. Its job is to assist in various metabolic reactions – particularly those involved in bile transport and bone development.
When it rises: A raised ALP most commonly signals one of two things:
bile duct obstruction (the bile flow is blocked) or accelerated bone activity (such as bone healing, growth, or bone disease).
Because ALP comes from two sources — liver and bone — doctors use GGT to distinguish between them.
If both ALP and GGT are raised together, the liver is almost certainly the source. If ALP is raised but GGT is normal, bone may be the cause.
Common causes of raised ALP:
Gallstones or bile duct blockage
Fatty liver disease
Liver inflammation (hepatitis)
Bone disorders (Paget’s disease, fractures in healing)
Pregnancy (ALP rises naturally in the third trimester)
GGT — Gamma Glutamyl Transferase
What it does: GGT is an enzyme found in high concentrations in liver cells and the bile duct lining. It helps transport amino acids and peptides across cell membranes — essentially acting as a gatekeeper at the liver cell surface.
When it rises: GGT is the most sensitive liver enzyme — meaning it reacts quickly and early to any liver stress.
It is often the first marker to rise, even before other enzymes change. It is particularly responsive to alcohol, medications, and fatty liver.
A raised GGT with normal ALP often simply reflects recent alcohol intake or medication effect — not necessarily serious liver disease.
SGOT — Aspartate Aminotransferase (AST)
What it does: SGOT is an enzyme that plays a key role in amino acid metabolism – specifically helping convert one amino acid into another to produce energy.
(Amino acids are the building blocks of proteins – the same proteins your body uses to build muscle, repair tissue, and carry out thousands of chemical reactions.) It is found in high quantities in liver cells, but also in heart muscle, skeletal muscle, and red blood cells.
When it rises: When liver cells or muscle cells are damaged, SGOT leaks into the bloodstream. Because it comes from multiple organs, a raised SGOT alone does not automatically confirm liver damage.
Intense exercise, a heart attack, or muscle injury can all raise SGOT without any liver involvement. This is why SGOT is always interpreted alongside SGPT, which is far more liver-specific.
Common causes of raised SGOT:
Liver inflammation (hepatitis, fatty liver)
Alcoholic liver disease
Heart attack or heart muscle damage
Intense physical exercise or muscle injury
Certain medications
SGPT — Alanine Aminotransferase (ALT)
What it does: SGPT is an enzyme involved in protein metabolism – helping convert stored energy into usable form for the body. Unlike SGOT, SGPT is found predominantly in liver cells, with very little present in other organs.
When it rises: This specificity makes SGPT the most reliable and closely watched marker of liver cell damage. When SGPT is raised, the liver is almost always the source. It rises with fatty liver disease, viral hepatitis, alcohol-related liver damage, and medication toxicity.
In India, a mildly raised SGPT — often between 45–80 U/L — is increasingly common due to the rising prevalence of non-alcoholic fatty liver disease (NAFLD), especially in people who do not drink alcohol.
Common causes of raised SGPT:
Non-alcoholic fatty liver disease (NAFLD) — the most common cause in India
The ratio between SGOT and SGPT is a simple but powerful diagnostic clue. It helps doctors narrow down the cause of liver enzyme elevation — not just confirm it exists.
Ratio
Pattern
What It Suggests
Below 1 (SGPT > SGOT)
SGPT higher
Fatty liver disease or viral hepatitis
Above 2 (SGOT >> SGPT)
SGOT much higher
Alcoholic liver disease (classical pattern)
1 to 2
Mixed
Various causes: interpret with the full clinical picture
The ratio is a guide, not a diagnosis. It is always read alongside symptoms, history, and other tests.
Proteins — What the Liver Manufactures
The liver is the body’s primary protein factory. The protein values on your LFT report tell your doctor how well the liver is producing, not just filtering.
Total Protein
Total protein is the sum of albumin and globulin in your blood.
In simple terms, albumin is the liver’s own protein, produced directly by the liver to maintain fluid balance and transport nutrients. Globulin is the immune system’s protein, made largely by immune cells to fight infection and disease.
Together, these proteins serve as building blocks for enzymes, hormones, immune cells, and the structural scaffolding of tissues.
A low total protein can indicate that the liver is struggling to produce enough, that the body is not absorbing adequate nutrition, or that protein is being lost through the kidneys.
Albumin
Albumin is the most abundant protein in the blood and the liver’s most important product.
It performs three critical jobs:
keeping fluid inside blood vessels (preventing leakage into surrounding tissues), transporting hormones, vitamins, calcium, and medications around the body, and maintaining blood pH balance.
Low albumin is one of the most reliable indicators of chronic liver disease.
When the liver is significantly damaged over time, its ability to manufacture albumin declines and fluid begins leaking out of blood vessels into the abdomen and legs, causing swelling.
Common causes of low albumin:
Chronic liver disease or cirrhosis
Malnutrition or prolonged fasting
Nephrotic syndrome (protein loss through kidneys)
Prolonged illness or inflammatory states
Globulin
Globulins are a group of proteins that include antibodies produced by the immune system. Unlike albumin, globulins are made largely by immune cells, not exclusively by the liver.
A raised globulin level can signal chronic infection, autoimmune disease, or liver cirrhosis (where the immune system becomes overactive in response to ongoing liver damage). A low globulin is less common but may suggest immune deficiency.
Albumin / Globulin (A/G) Ratio
The A/G ratio reflects the balance between these two protein groups.
A healthy liver produces more albumin than globulin, keeping this ratio above 1.
When the liver is damaged chronically, albumin production falls. Simultaneously, the immune system ramps up globulin production in response to the ongoing injury.
This combination drives the ratio downward, and a low A/G ratio is often a signal of chronic liver disease, ongoing inflammation, or autoimmune conditions.
What Can Affect Your LFT Results?
Several factors can temporarily alter your LFT, independent of true liver disease. Always inform your doctor about these before your report is interpreted:
Medications: paracetamol, statins, anti-TB drugs, antifungals, and many herbal supplements can raise liver enzymes
Alcohol: even moderate intake within 24–48 hours can elevate GGT and SGOT
Strenuous exercise: raises SGOT through muscle breakdown, not liver injury
Fatty liver disease: one of the most common causes of mildly raised SGPT and GGT in India
Pregnancy: ALP rises naturally in the third trimester
Recent viral illness: can transiently elevate liver enzymes
Malnutrition or prolonged fasting: can lower albumin and total protein
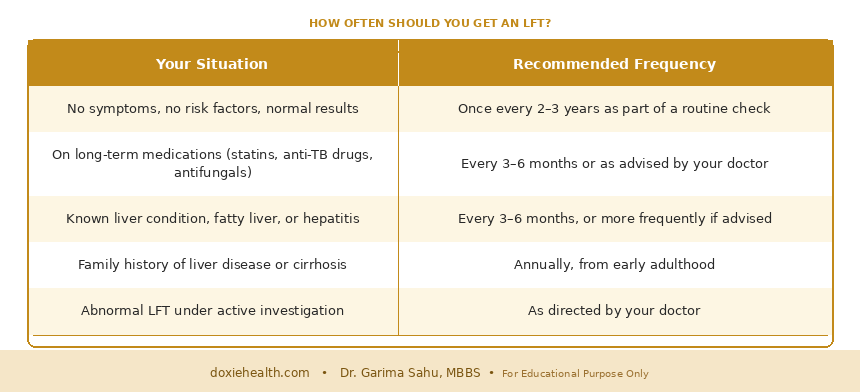
How Often Should You Get an LFT?
Image: DoxieHealth | How often should you get a liver function test?
👩⚕️ Doctor’s Note: An LFT rarely tells the whole story on its own. Mildly raised enzyme, particularly SGPT, is extremely common and often caused by fatty liver, which is reversible with lifestyle changes. What matters is the pattern of results, how far above normal the values are, and your overall clinical picture. One abnormal number is not a diagnosis, context is everything.
When Should You Be Concerned?
Contact your doctor promptly if your LFT shows:
SGPT or SGOT is more than 3 times the upper limit of normal
Raised bilirubin with yellowing of skin or eyes
Low albumin alongside swelling in the legs or abdomen
ALP and GGT are both elevated with persistent right-sided abdominal pain
Any values worsening on repeat testing
Mild, isolated elevations, particularly a slightly raised SGPT, are common and often not alarming. Always interpret results with your doctor.
The Takeaway
Your liver function test is a window into one of your body’s most vital organs. Understanding what each value means helps you walk into your doctor’s appointment prepared, not anxious.
If your LFT came back with raised values, the most important next step is context – discussing the pattern of results with your doctor, not searching for a diagnosis alone. For a broader picture of your health, you may also want to read our guides on the Lipid Profile and the Complete Blood Count (CBC) on DoxieHealth.
Questions to Ask Your Doctor
Could any of my medications or supplements be affecting my LFT results?
Do I need to repeat this test, or are further investigations required?
Could fatty liver disease be contributing to my raised enzymes?
Should I make any lifestyle or dietary changes based on these results?
References
Kasper DL, Fauci AS, et al. Harrison’s Principles of Internal Medicine, 21st ed. McGraw-Hill Education; 2022.
Kumar V, Abbas AK, Aster JC. Robbins & Cotran Pathologic Basis of Disease, 10th ed. Elsevier; 2020.
⚠️ Medical Disclaimer This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice


 Explained")


Leave a Reply