Do you feel constantly tired, gain weight without explanation, or feel your heart racing for no reason? Has your hair been falling out more than usual, or do you feel cold when everyone else is comfortable? These symptoms are easy to dismiss — but they are frequently the first signs that your thyroid gland is not functioning as it should. A simple blood test — the thyroid function test – can answer these questions in hours.
This article explains what TSH, T3, and T4 measure, how to read your thyroid report, what abnormal values mean, and how thyroid dysfunction connects to cholesterol, anaemia, fertility, and other conditions you may already be managing.
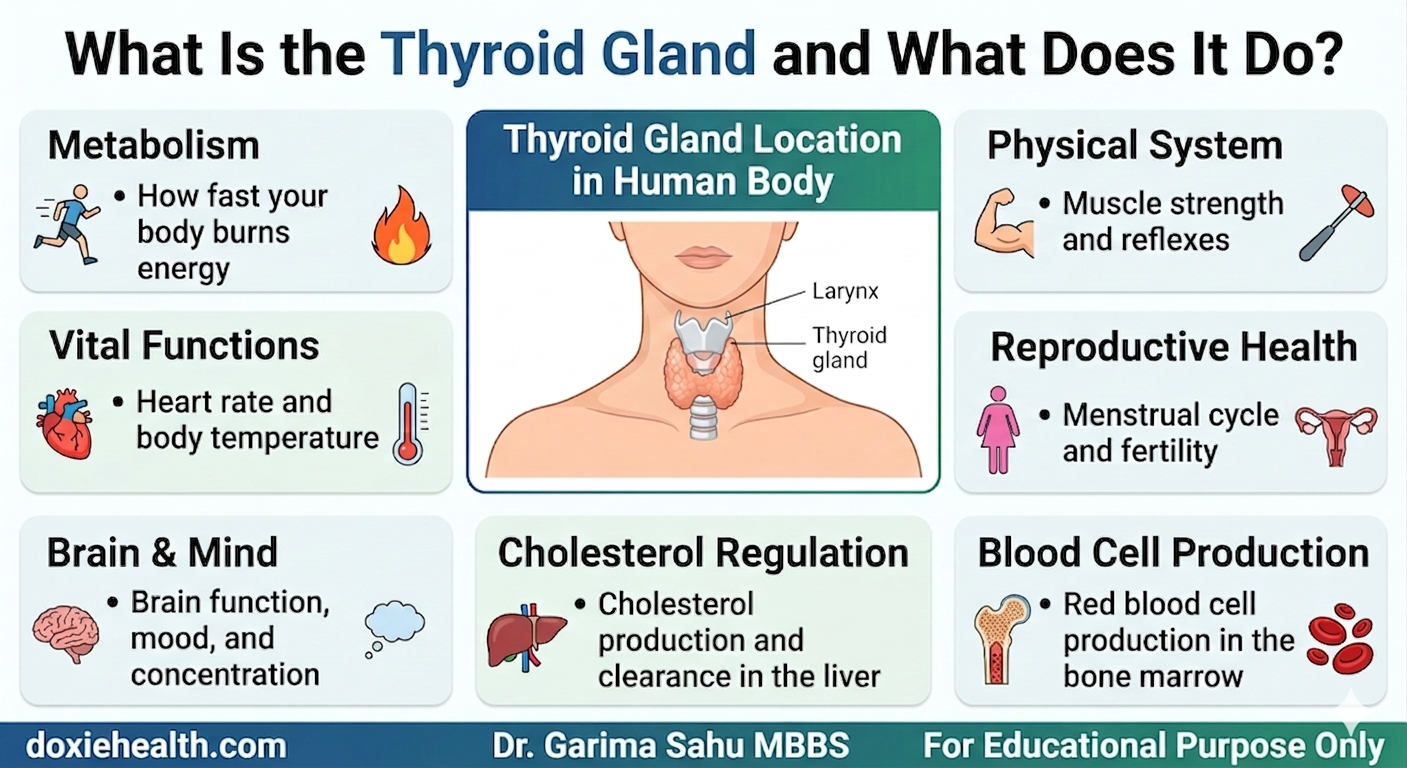
What Is the Thyroid Gland and What Does It Do? | Dr. Garima Sahu, MBBS — DoxieHealth
The thyroid is a small, butterfly-shaped gland sitting at the base of the neck. Despite its size, it controls the metabolic rate of almost every cell in the body.
When the thyroid produces too little hormone, i.e. known as hypothyroidism, every process in your body slows down.
When it produces too much hormone, i.e. known as hyperthyroidism, everything accelerates.
Both states affect multiple organ systems simultaneously.
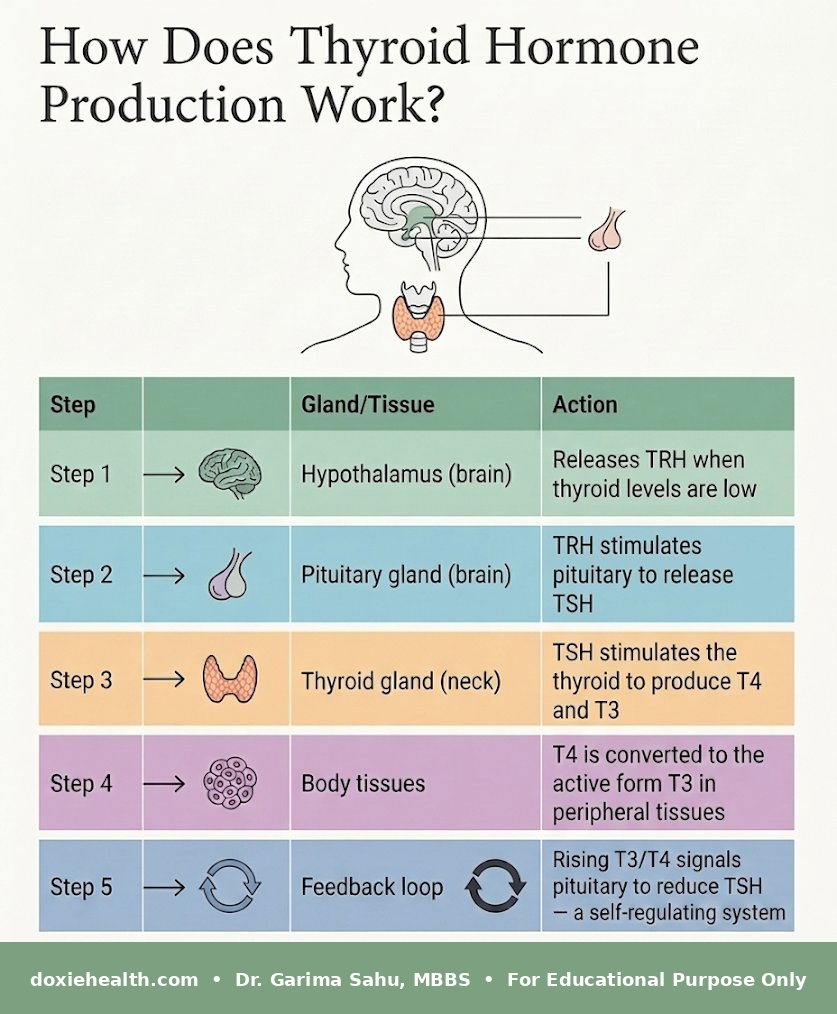
How Does Thyroid Hormone Production Work?
How thyroid hormone production works — the hypothalamus-pituitary-thyroid (HPT) axis explained step-by-step. Doxiehealth
Key insight TSH moves in the opposite direction to thyroid hormones. When thyroid hormones are low, TSH rises. When thyroid hormones are high, TSH falls. This is why TSH is the most sensitive and reliable first-line marker for thyroid dysfunction.
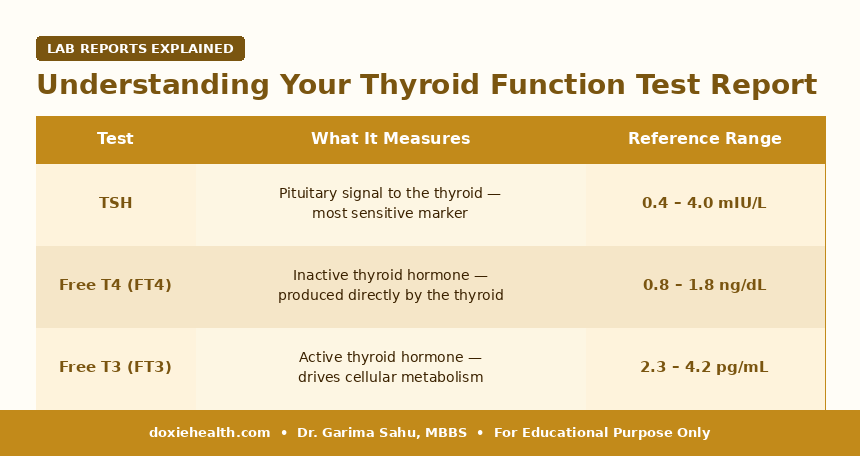
Understanding Your Thyroid Function Test Report
The three main values in your report
Thyroid Function Test Reference Ranges | Dr. Garima Sahu, MBBS — DoxieHealth
Free vs Total Your report may show Free or Total T3/T4. Free values measure only the unbound, biologically active hormone. Total values include both bound and unbound hormone and are less clinically useful. Most modern labs use Free T3 and Free T4.
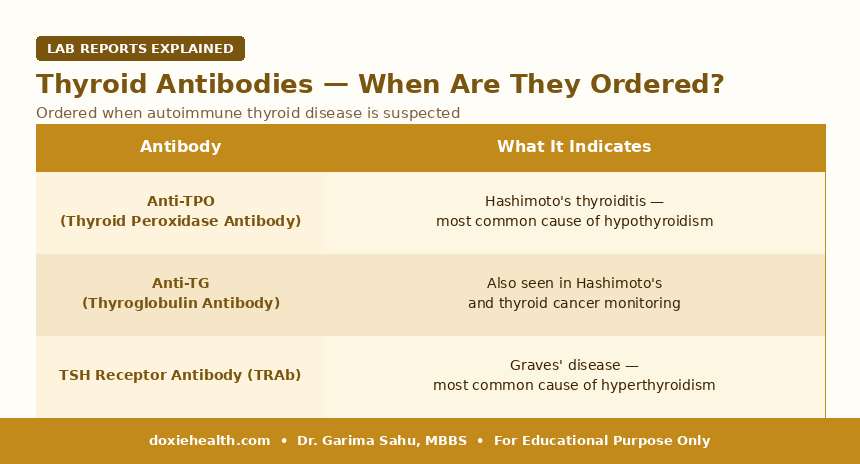
Thyroid antibodies — when are they ordered?
Thyroid Antibodies — When Are They Ordered? | Dr. Garima Sahu, MBBS — DoxieHealth
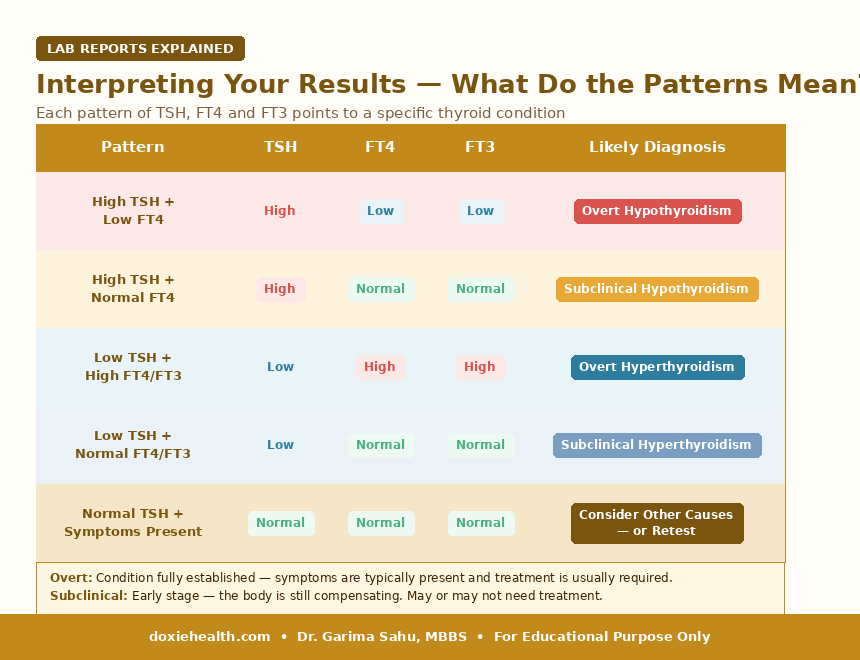
Interpreting Your Results — What Do the Patterns Mean?
Thyroid Result Patterns & Diagnosis | Dr. Garima Sahu, MBBS — DoxieHealth
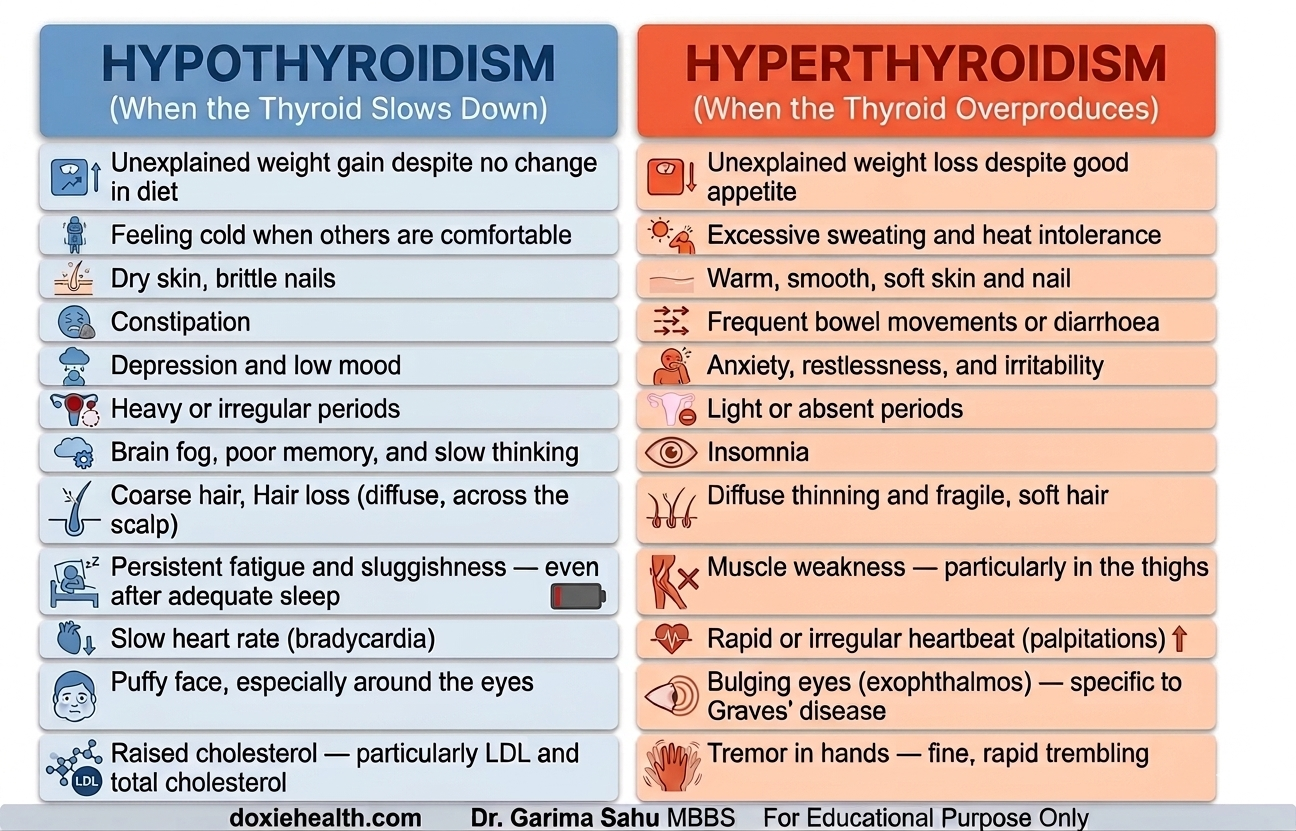
Hypothyroidism vs. Hyperthyroidism – Recognising the Symptoms
The symptoms of these two conditions point in opposite directions — here’s how to tell them apart:
A comparison chart of common symptoms for Hypothyroidism and Hyperthyroidism.
Hypothyroidism — When the Thyroid Slows Down
Hypothyroidism is the most common thyroid disorder in India — affecting an estimated 1 in 10 adults, with women affected 5-8 times more than men.
Brief management
Treated with levothyroxine – a synthetic T4 tablet taken daily on an empty stomach, 30-60 minutes before breakfast.
Dose is individualised based on TSH levels, body weight, age, and pregnancy status. TSH is rechecked every 6-8 weeks after dose changes until stable, then annually. Most patients require lifelong treatment.
Hyperthyroidism — When the Thyroid Overproduces
Hyperthyroidism is far less common than hypothyroidism in India, affecting an estimated 1–2% of the population. Unlike hypothyroidism, it affects men and women more equally, with Graves’ disease being the most common cause.
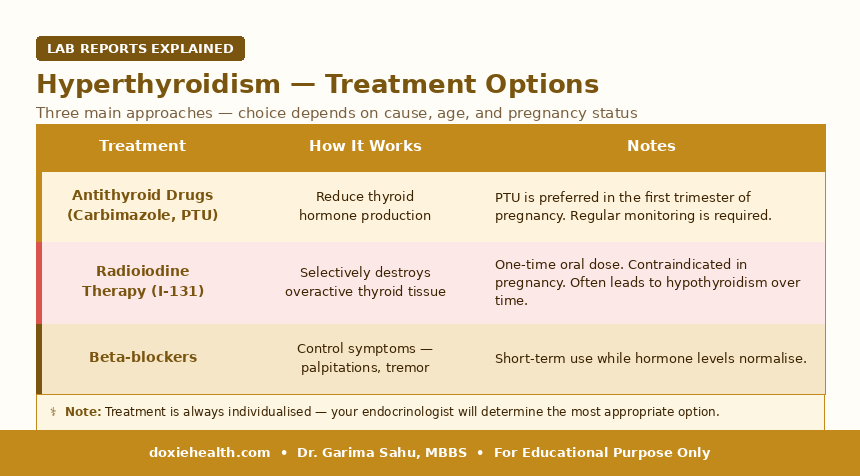
Brief management
Hyperthyroidism Treatment Options | Dr. Garima Sahu, MBBS — DoxieHealth
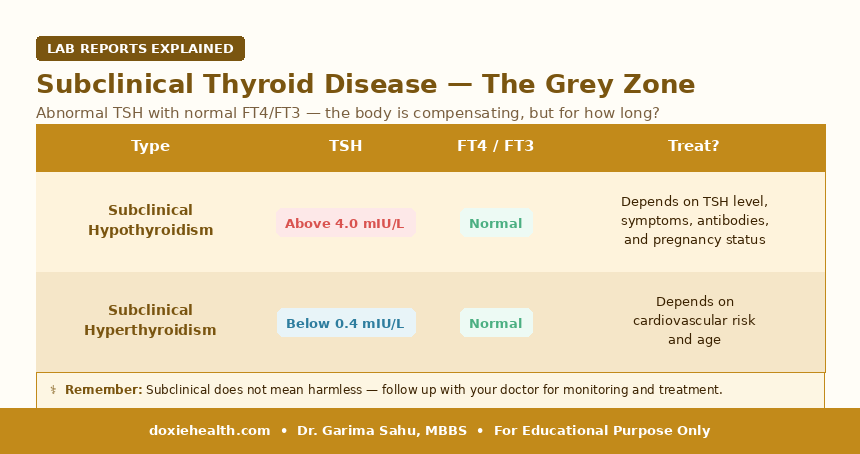
Subclinical Thyroid Disease -The Grey Zone
Subclinical thyroid dysfunction occurs when TSH is abnormal, but T3 and T4 remain within normal range. Extremely common in India and frequently discovered incidentally.
Subclinical Thyroid Disease — The Grey Zone | Dr. Garima Sahu, MBBS — DoxieHealth
Why it matters: Even subclinical hypothyroidism – particularly if TSH is above 10 mIU/L or anti-TPO antibodies are positive — is associated with raised cholesterol, increased cardiovascular risk, and progression to overt hypothyroidism. Always discuss with your doctor rather than dismissing it as borderline.
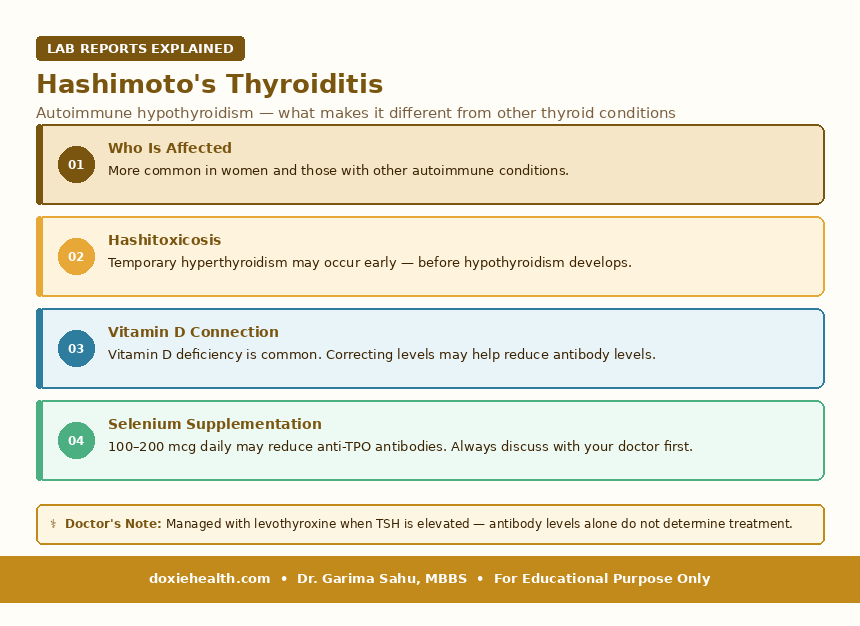
Hashimoto’s is the most common cause of hypothyroidism in India. The immune system produces antibodies (primarily anti-TPO) that attack the thyroid gland, causing progressive destruction and declining hormone production.
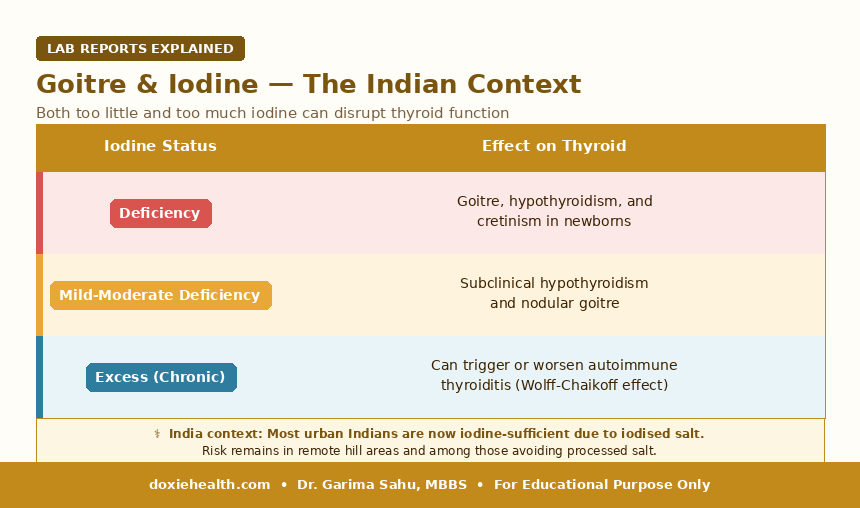
A goitre is an enlargement of the thyroid gland — visible as a swelling at the base of the neck. Both too little and too much iodine can cause thyroid problems:
Goitre & Iodine — The Indian Context | Dr. Garima Sahu, MBBS — DoxieHealth
Practical note Universal salt iodisation has dramatically reduced iodine deficiency in India. Use iodised salt in normal cooking quantities. Do not supplement iodine without medical guidance — excess iodine can paradoxically suppress thyroid function.
Thyroid and Other Conditions- The Connections
Condition
Connection
Read more
High cholesterol
Hypothyroidism reduces hepatic LDL receptor activity, raising LDL. Always check TSH before starting a statin.
B12 deficiency and hypothyroidism frequently coexist; both cause fatigue, brain fog, and depression. Always check both together.
B12 article
Fertility
Both hypothyroidism and hyperthyroidism disrupt the menstrual cycle and ovulation. TSH should be part of every fertility workup.
—
Pregnancy
Untreated thyroid dysfunction carries serious risks. Levothyroxine doses increase 25-30% in pregnancy. TSH target: 0.1-2.5 mIU/L in the first trimester.
—
How Often Should You Test?
No risk factors + normal TSH
Once every 3-5 years as part of routine preventive screening. Annual testing is recommended for women over 35, those with a family history of thyroid disease, or those with other autoimmune conditions.
Family history of thyroid, diabetes, or metabolic disease
TSH annually — thyroid dysfunction clusters in families and frequently coexists with metabolic disorders, including Type 2 diabetes, insulin resistance, and metabolic syndrome.
If a first-degree relative has thyroid disease or metabolic syndrome, do not wait for symptoms before testing.
Risk factors present or abnormal values
Subclinical hypothyroidism without treatment: every 6-12 months
On levothyroxine — stable dose: TSH annually
On levothyroxine — dose recently changed: recheck TSH in 6-8 weeks
On antithyroid drugs: TFT every 4-6 weeks during dose titration, then every 3 months
Pregnancy: TSH every trimester — or more frequently if on treatment
Hashimoto’s with positive antibodies: TSH annually minimum
Family history of thyroid disease, diabetes, or metabolic syndrome: TSH annually
Key Clinical Insights
TSH is the best first-line test — not T3 or T4 alone.
A normal TSH with persistent symptoms warrants repeating the full panel.
Always check anti-TPO if TSH is elevated
It identifies Hashimoto’s, predicts progression, and changes management.
Biotin supplements falsely lower TSH on immunoassay-based tests
Stop biotin for 48-72 hours before a thyroid blood test.
TSH varies by time of day — it is highest in the early morning.
For consistent monitoring, always test at the same time of day.
Do not self-adjust the levothyroxine dose
Even small changes significantly affect TSH. Always adjust under medical guidance.
Soy, calcium, and iron supplements interfere with levothyroxine absorption
Take levothyroxine at least 4 hours apart from these.
Doctor’s Note The thyroid is one of the most under-checked glands in Indian clinical practice, particularly in women presenting with fatigue, weight gain, or hair loss.A TSH test costs under Rs. 300, takes minutes, and can explain symptoms that have been dismissed for years. If you have any of the symptoms described in this article — and especially if you are a woman over 25, pregnant, or have a family history of thyroid or metabolic disease — ask for a TSH test at your next routine blood work.
When Should You Be Concerned? TSH above 10 mIU/L — even if T3/T4 are normal. TSH suppressed below 0.1 mIU/L — risk of atrial fibrillation and bone loss. Visible neck swelling or a lump in the thyroid area. Pregnant or planning pregnancy, and TSH has not been checked. On levothyroxine, symptoms are returning despite being told TSH is normal. Palpitations, tremor, or unexplained weight loss — rule out hyperthyroidism promptly.
The Takeaway
The thyroid function test is one of the most clinically informative blood tests available and one of the most underutilised in preventive health in India.
TSH is the single most sensitive marker for thyroid dysfunction.
Understanding your result and the pattern of TSH, FT4, and FT3 together tells you not just whether your thyroid is abnormal, but what type of dysfunction is present and what it means for your overall health.
Dedicated articles on hypothyroidism and hyperthyroidism — covering diagnosis, treatment, and long-term management in detail — are coming soon on DoxieHealth.
Questions to Ask Your Doctor
My TSH is slightly elevated – do I need treatment or just monitoring?
Should anti-TPO antibodies be checked alongside my TSH?
I am on levothyroxine – is my current dose correct for my age and weight?
I am planning a pregnancy – what TSH level should I aim for before conceiving?
My cholesterol is high – could my thyroid be contributing?
Should I check my Vitamin D, B12, and CBC alongside my thyroid test?
References
1. Garber JR et al. Clinical Practice Guidelines for Hypothyroidism in Adults. Thyroid. 2012;22(12):1200-1235. Read here →
2. Ross DS et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism. Thyroid. 2016;26(10):1343-1421. Read here →
3. Unnikrishnan AG et al. Prevalence of Hypothyroidism in Adults: An Epidemiological Study in Eight Cities of India. Indian Journal of Endocrinology and Metabolism. 2013;17(4):647-652. Read here →
4. Maraka S et al. Subclinical Hypothyroidism in Women Planning Conception and During Pregnancy. Read here →
5. Harrison’s Principles of Internal Medicine, 21st Edition. McGraw-Hill, 2022.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice

 Explained")


Leave a Reply