You got a KFT blood test done – maybe as part of a routine health check, or because your doctor wanted to monitor your diabetes or blood pressure. And somewhere on that report, you see words like creatinine, BUN, urea, uric acid. The numbers are there, the reference range is printed right next to them, but it still feels like you are reading a report in a language you were never taught.
That is exactly why this article exists. The Kidney Function Test/Renal Function Test – commonly called KFT or RFT – is one of the most routinely ordered blood panels in India. It tells your doctor how well your kidneys are doing their job. And once you understand what each parameter is actually measuring, the report stops feeling overwhelming and starts making sense.
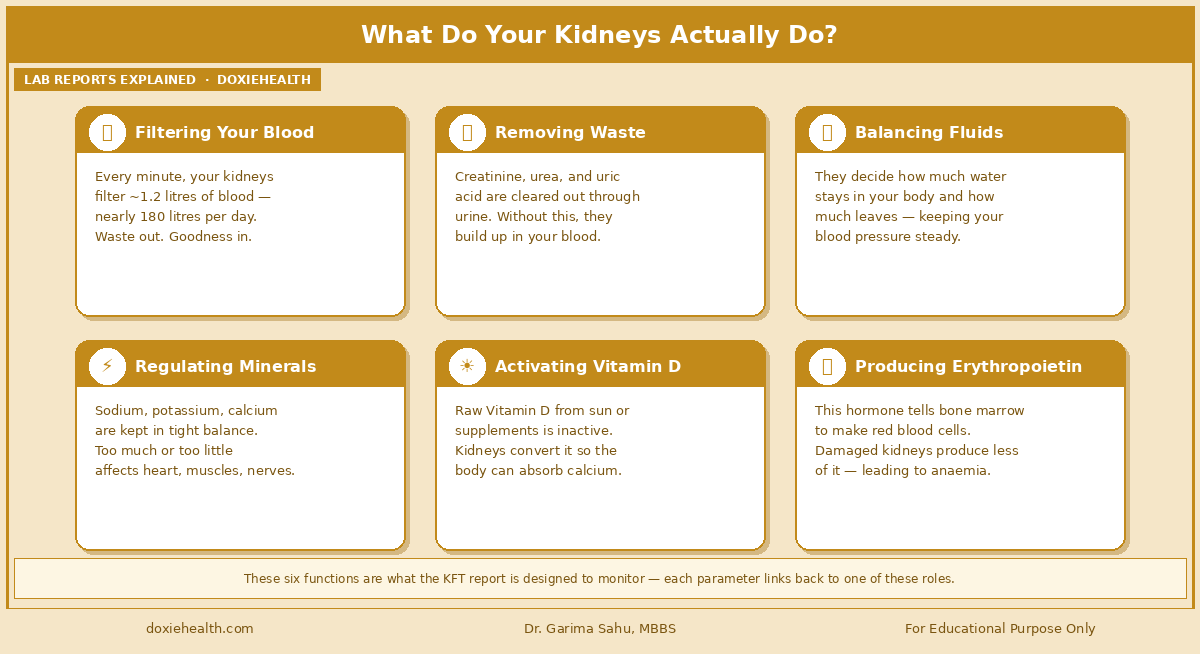
Before we look at the numbers, it helps to understand what the kidneys are responsible for. Most people know that kidneys make urine. But that is just one part of a much bigger job. Your kidneys work silently, around the clock. Here is what they are doing every single day:
The six core functions your kidneys perform every day. Image: DoxieHealth
Think of your kidneys like the municipal water treatment plant of your body. They filter out waste, regulate what flows through, maintain the right chemical balance, and keep everything running at steady pressure. The KFT is essentially the inspection report for that plant.
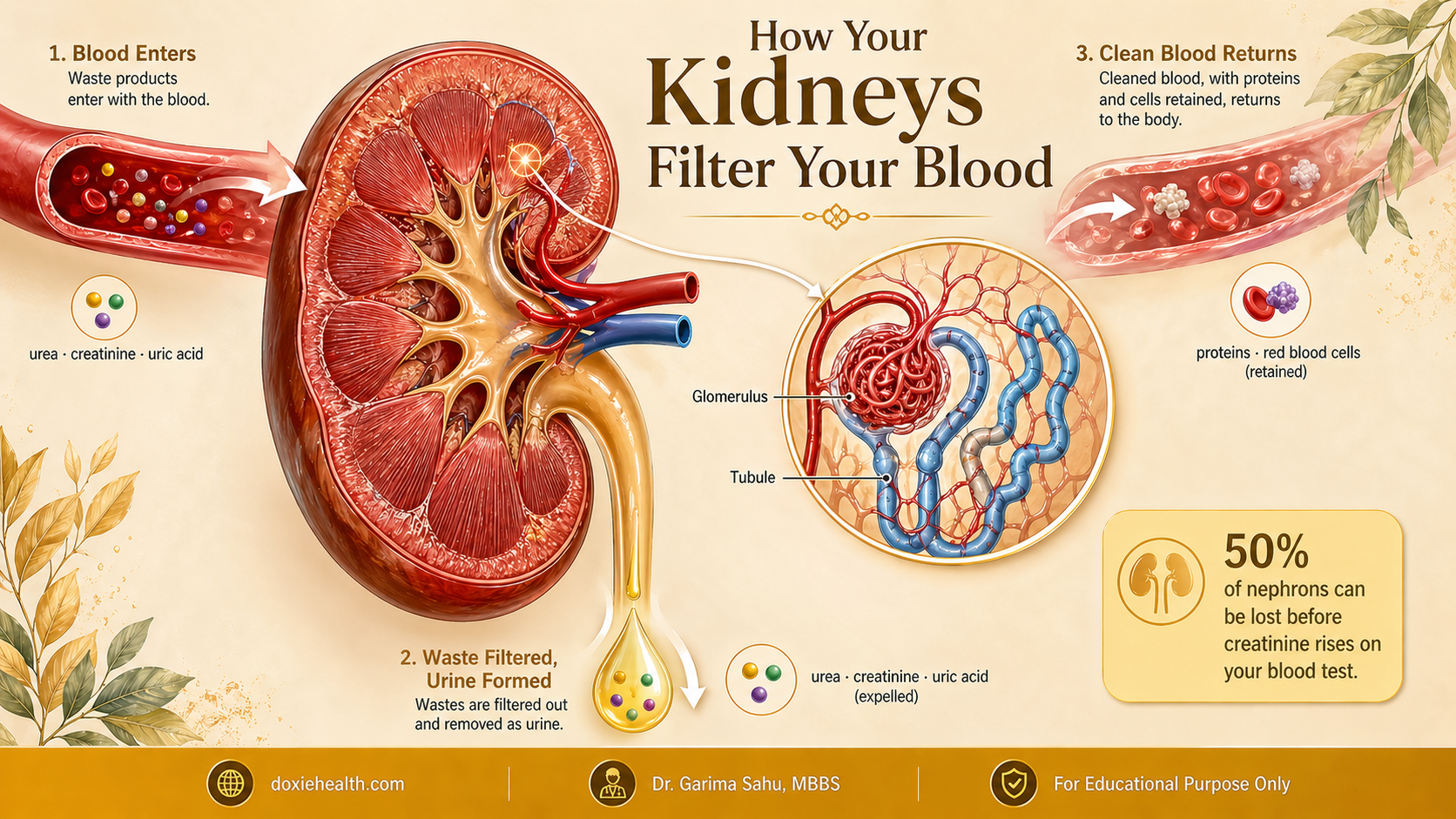
How Do Kidneys Filter Your Blood?
How your kidneys filter blood — from waste entering with the blood to clean blood returning and urine forming. Image: DoxieHealth
Inside each kidney, there are approximately one million tiny filtering units called nephrons. Each nephron has two main parts: a tiny ball of blood vessels called the glomerulus, and a long winding tube called the tubule.
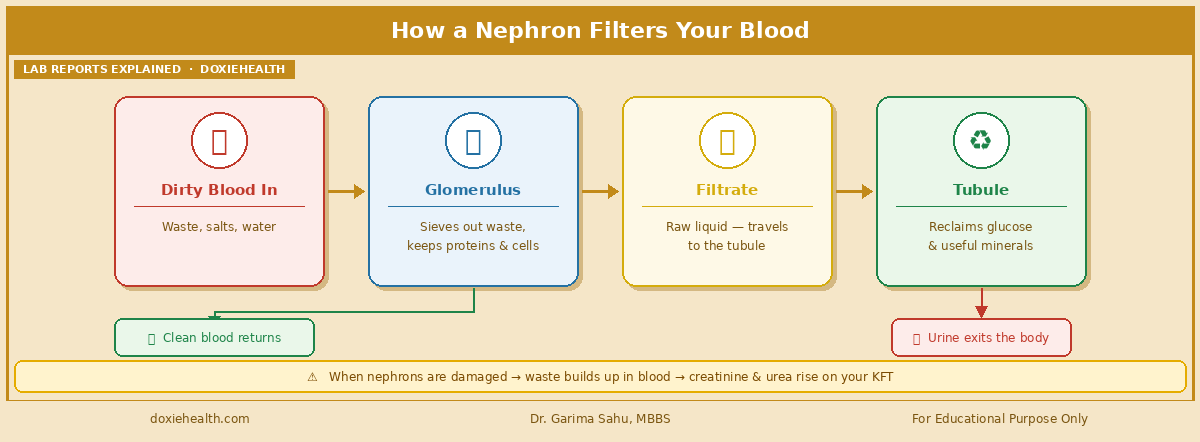
Here is how it works.
How a nephron filters your blood — from dirty blood in to clean blood and urine out. Image: DoxieHealth
When the glomerulus or tubule is damaged, this process breaks down. Waste products that should be eliminated in the urine instead accumulate in the blood. That is when creatinine, urea, and BUN levels begin to rise on your report.
Here is an important detail your doctor knows: the kidneys have significant reserve capacity. They can continue functioning with only 50% of their nephrons intact, and creatinine may still appear normal. This is why kidney disease often has no symptoms in its early stages, and why a KFT is such an important screening tool for anyone at risk.
Your KFT Report at a Glance
Reference ranges from Harrison’s Principles of Internal Medicine, 21st Edition. Your lab’s printed reference interval takes priority.
Parameter
Harrison’s Range
Units
What It Measures
Blood Urea Nitrogen (BUN)
8 – 20
mg/dL
Nitrogen from urea in blood
Urea (Calculated)
17 – 43
mg/dL
Total urea in blood
Serum Creatinine
0.7-1.3 (M) / 0.6-1.1 (F)
mg/dL
Muscle waste filtered by kidneys
BUN / Creatinine Ratio
9:1 – 23:1
Ratio
Helps locate source of kidney stress
Urea / Creatinine Ratio
Less than 52
Ratio
Cross-check of urea-creatinine balance
Calcium
8.5 – 10.5
mg/dL
Bone-kidney mineral regulation
Uric Acid
3.5-7.2 (M) / 2.6-6.0 (F)
mg/dL
Purine breakdown product
What Each Parameter Means
1. Blood Urea Nitrogen (BUN) and Urea (Calculated)
Protein does not just disappear after a meal. Your body breaks it down, uses what it can, and whatever is left behind becomes waste, which travels to the liver, and gets converted into a safe, water-soluble compound called urea and released into the blood — ready to be flushed out by the kidneys through urine.
Now, protein is made of nitrogen. So when protein breaks down, nitrogen is released as part of that waste.
BUN — Blood Urea Nitrogen — simply measures how much of that nitrogen waste is floating in your blood right now. The Calculated Urea on your report is just the same value expressed differently, like two people describing the same traffic jam — one says 5 kilometres, the other says 3 miles. Same waste, different words.
When kidneys are functioning well, BUN and urea stay within range. When the kidneys slow down, or when there is more protein waste than usual, these values rise.
BUN / Urea is HIGH when:
Reduced kidney function: waste is not being cleared efficiently, so urea accumulates in the blood
Dehydration: less fluid in the body concentrates the blood, making waste levels appear higher
High protein diet or large non-veg meal before the test: more protein breakdown means more urea is produced
Gastrointestinal bleeding: blood in the gut is digested like protein, adding a large nitrogen load and raising BUN significantly
Catabolic states: fever, major infection, surgery, or trauma all break down more body tissue than usual, producing extra waste
BUN / Urea is LOW when:
Liver disease: the liver cannot produce urea normally, so less enters the blood
Very low protein intake: severe malnutrition or extremely restrictive diets reduce urea production at the source
Overhydration: excess fluids dilute the blood, lowering the concentration of all waste markers
2. Serum Creatinine
If BUN is the variable one, creatinine is the steady one. And that steadiness is exactly what makes it the most reliable marker on your KFT.
Your muscles run on energy. And like any engine, they produce a little waste when they work. That waste is called creatinine. The amount your body makes each day is very consistent — it does not change much with your diet or daily routine (can be increased slightly after dehydration and high-intensity exercise, which your doctor will clarify with you). Because of this predictability, the kidneys are expected to clear a fixed amount of creatinine every single day.
When kidney filtration drops, creatinine starts to accumulate. And because production is stable, a rising creatinine is a reliable sign that the kidneys are struggling – not that your diet changed or you had a big meal. This is the most important single number on your KFT report.
Creatinine is HIGH when:
Reduced kidney function: the kidneys cannot clear creatinine at their normal rate, so it builds up
Dehydration: reduced blood flow to the kidneys slows filtration, even when the kidneys themselves are healthy
Regular NSAID use: ibuprofen, diclofenac, and nimesulide reduce blood flow to the kidney’s filtration units
Intense exercise just before the test: muscles release extra creatinine during heavy workouts, temporarily raising levels
Creatine or protein supplement use: high intake over time raises baseline creatinine production in muscles
Certain medications, such as trimethoprim and cimetidine, can block creatinine secretion and raise levels without any true kidney damage
Creatinine is LOW when:
Very low muscle mass: elderly patients, those who are bedridden, or severely malnourished individuals produce less creatinine, so their levels may appear normal even if kidney function is reduced – this is an important limitation that your doctor accounts for
Pregnancy: The kidneys filter more efficiently during pregnancy, and creatinine is naturally diluted
Many Indian labs now calculate and print the eGFR (Estimated Glomerular Filtration Rate) alongside creatinine. This value tells you how many millilitres of blood the kidneys are filtering per minute. An eGFR above 90 is considered normal. If your lab has printed this value and it is below 60, that is worth a dedicated conversation with your doctor.
3. BUN / Creatinine Ratio
This ratio does not tell you how bad kidney function is. It tells your doctor why the values may be elevated – specifically, where the problem is coming from. Normal range: 9:1 to 23:1.
Ratio Pattern
Interpretation
What It Suggests
HIGH Ratio (above 23)
BUN elevated, creatinine near-normal
Pre-renal
LOW Ratio (below 9)
creatinine elevated
Intrinsic kidney damage
Ratio stays in normal range (9-23)
Both BUN and creatinine elevated,
Intrinsic kidney disease at a more advanced stage
Pre-renal: The kidney itself is fine – the supply line is blocked. There is not enough blood reaching the kidneys (dehydration, heart failure, blood loss).
Intrinsic kidney damage: the kidney tissue itself is affected and fails to clear creatinine properly.
Intrinsic kidney disease at a more advanced stage: Both BUN and creatinine are rising together, at the same pace. This usually means the kidney itself is gradually losing its ability to filter — not a temporary issue like dehydration, but a steady decline. Your doctor will track this across multiple tests over time to confirm the pattern.
Think of it using the RO purifier analogy again. If the purifier is producing less water because the supply line has low pressure, the machine itself is fine – that is a pre-renal problem. If the filter membrane inside is torn or clogged, the input is fine, but the machine is damaged – that is, intrinsic kidney damage. If both input and output are reduced proportionally, the whole system is wearing out.
4. Urea / Creatinine Ratio
This is a cross-check that reinforces the interpretation of the BUN/creatinine ratio.
A ratio below 52 is expected. It is most useful when read alongside BUN, creatinine, and the BUN/creatinine ratio to build a complete picture.
Ratio is HIGH when:
Dehydration: concentrating waste products in the blood raises urea disproportionately
Very high protein intake: raising urea production more than creatinine
Gastrointestinal bleeding: contributing extra nitrogen load from digested blood
Ratio is LOW when:
Severe reduction in kidney filtration: affecting creatinine more than urea
Very low protein intake: reducing urea production while creatinine stays relatively stable
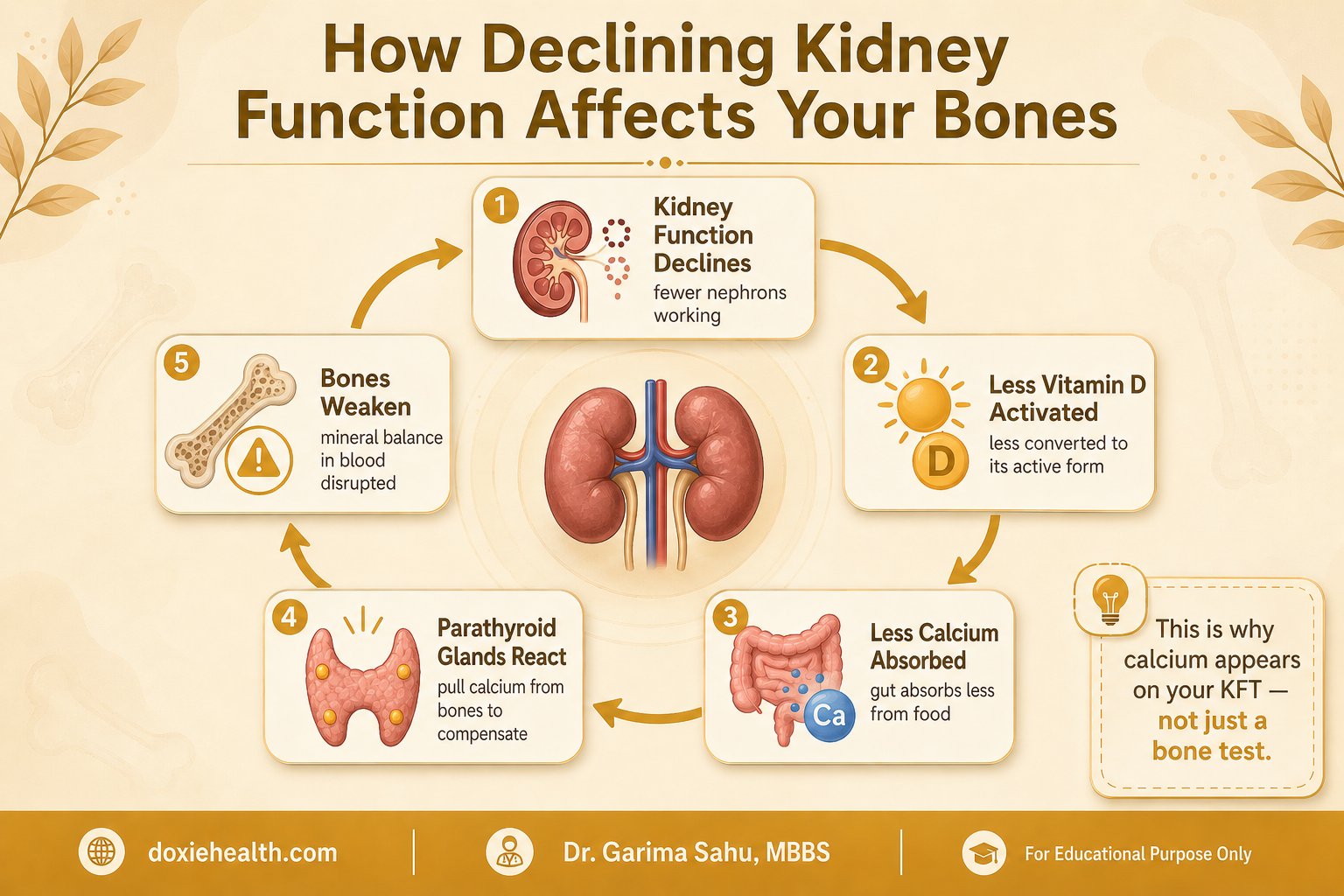
5. Calcium
Most people think calcium is just about strong bones. But the calcium circulating in your blood is doing something far more urgent — it keeps your heart beating rhythmically, your nerves firing correctly, and your blood clotting when you need it to. Too little or too much, even briefly, and the body feels it immediately.
Keeping blood calcium in a precise range is a three-way job — your kidneys, Vitamin D, and a hormone called PTH (parathyroid hormone) all work together to maintain that balance around the clock.
When kidneys lose function, a chain reaction begins — less Vitamin D, less calcium absorbed, and eventually weaker bones. This is why calcium appears on your KFT report. Image: DoxieHealth
See our Vitamin D article for a full breakdown of deficiency signs and optimal ranges.
Overactive parathyroid glands (hyperparathyroidism): pulling excess calcium out of bones into the blood
Excessive Vitamin D supplementation: driving too much calcium absorption from the gut
Certain cancers, such as lung, breast, and myeloma, can release substances that raise blood calcium
Prolonged immobilisation: causes calcium to leach from bones into the blood
Calcium is LOW when:
Declining kidney function: less active Vitamin D is produced, reducing calcium absorption from food
Vitamin D deficiency: from diet or lack of sunlight exposure, reducing gut absorption
Very low magnesium: magnesium is needed for PTH to work properly; if magnesium is low, PTH cannot maintain calcium levels
Certain medications: including some used for osteoporosis and seizures
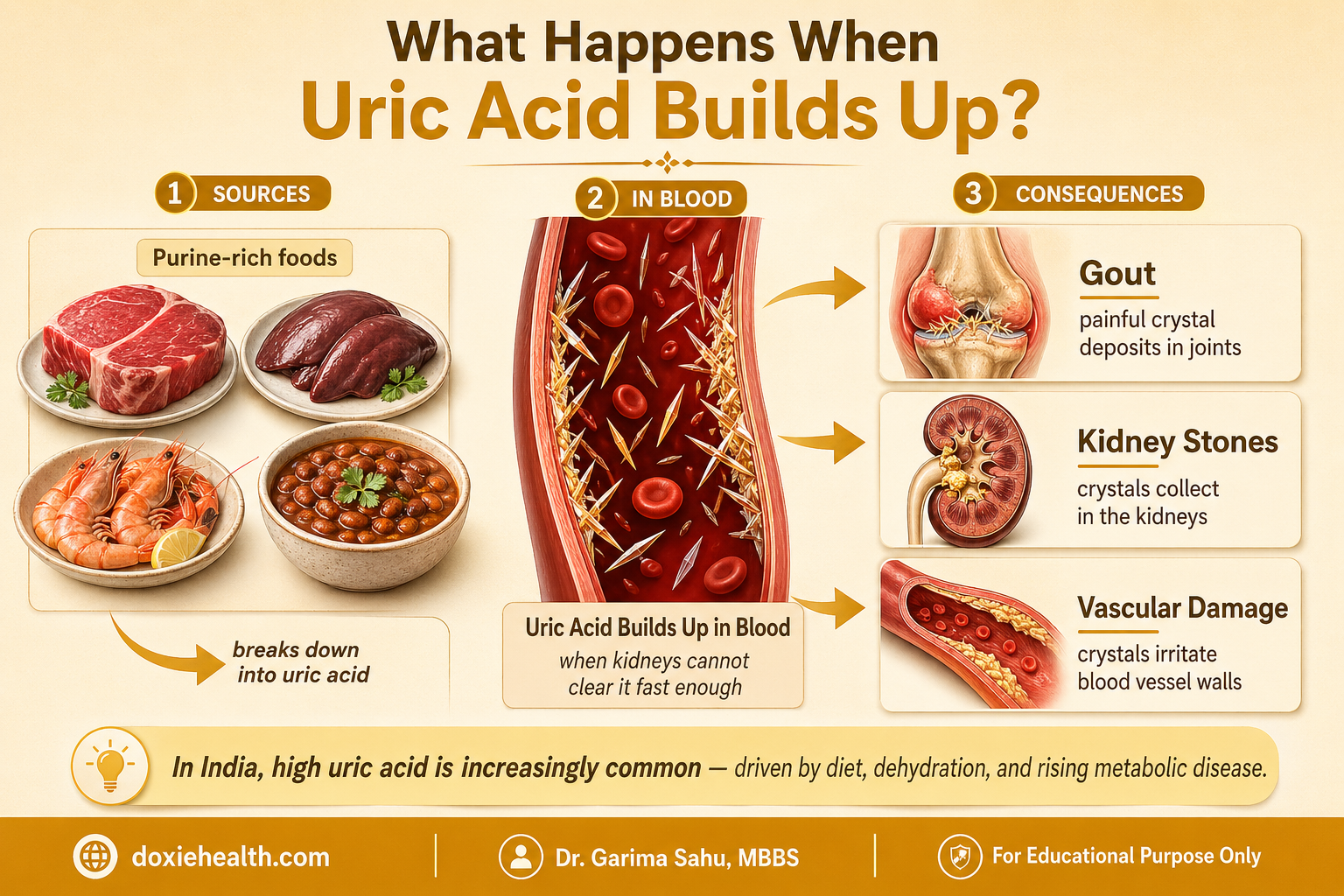
6. Uric Acid
Every time your body breaks down purine-rich foods — red meat, organ meats, shellfish, or certain lentils and legumes (masoor dal, Urad dal and rajma) — it producesa waste product calleduric acid. Under normal circumstances, about 70% of uric acid is cleared by the kidneys through urine, and the rest is excreted through the gut.
When uric acid builds up faster than the kidneys can clear it, it begins to deposit in joints, kidneys, and blood vessels. Image: DoxieHealth
This is closely linked to the conditions we cover in our Lipid Profile article.
High purine diet: red meat, organ meats, shellfish, and certain lentils increase uric acid production
Reduced kidney function: clearance is impaired, and uric acid accumulates in the blood
Dehydration: concentrates uric acid in the blood
Rapid cell breakdown: as in cancer treatment or severe infections, large amounts of cell material are broken down quickly
Certain medications: low-dose aspirin, some diuretics, and anti-TB drugs are known to raise uric acid levels
Metabolic syndrome and obesity are both strongly linked to elevated uric acid
Uric Acid is LOW when:
Allopurinol or losartan use: these medications actively lower uric acid as part of their action
Very low purine diet over a long period: uncommon, and a low uric acid is rarely a clinical concern on its own
What Can Affect Your KFT Results?
Before your doctor concludes that a value is abnormal, they will consider whether any of these common factors may have shifted your results:
Factor
Parameter Affected
Direction
Why It Matters
Dehydration before the test
BUN, Creatinine, Urea
HIGH
Most common pre-test factor in India
Large non-veg or high-protein meal
BUN, Urea
HIGH
Fast before the test if advised
Intense exercise just before the test
Creatinine, Uric Acid
HIGH
Muscles release extra creatinine
Regular NSAID use (ibuprofen, diclofenac)
Creatinine, BUN
HIGH
Restricts blood flow to kidneys
Ayurvedic or herbal supplements
Creatinine, BUN
HIGH
Some are nephrotoxic – tell your doctor
Very low muscle mass (elderly, malnourished)
Creatinine
FALSE LOW
Can mask reduced kidney function
Excess Vitamin D supplementation
Calcium
HIGH
Check dose with your doctor
Creatine supplements (young men)
Creatinine
HIGH
Common and often overlooked
This is why your doctor will always ask about recent activity, diet, and medications before interpreting a KFT.
A slightly elevated creatinine after a gym session in a healthy 28-year-old is a very different finding from the same number in a 58-year-old with long-standing diabetes.
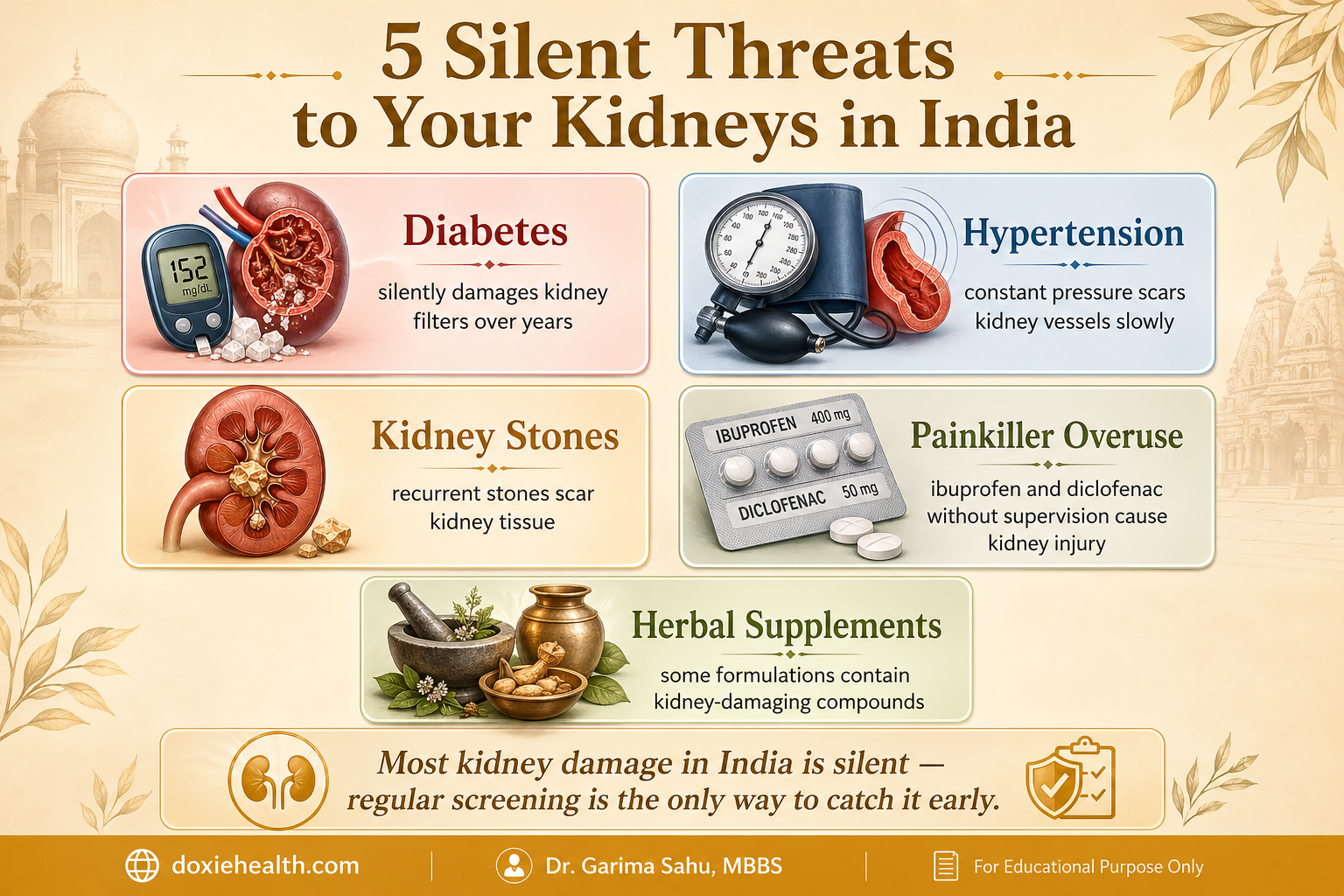
India-Specific Context: Who Needs to Pay Extra Attention
India carries one of the highest burdens of chronic kidney disease in the world. Several conditions common in India make kidney monitoring particularly important.
Most kidney damage in India happens silently over years. These are the five most common reasons your kidneys may be under stress without you knowing it. Image: DoxieHealth
Diabetes is the leading cause of kidney failure in India. High blood sugar silently damages kidney filters over the years.
Get a KFT and urine albumin test at least once a year.
Hypertension constant pressure, scars the kidney blood vessels slowly. Many patients only discover the damage when creatinine is already elevated.
Kidney stones, recurrent stones scar kidney tissue and are strongly linked to high uric acid. A high uric acid level with a history of stones needs a plan, not just monitoring.
NSAID overuse is a significant, underreported cause of kidney damage in India.
Diclofenac, ibuprofen, and nimesulide are available without prescription across India. Occasional use is fine. Regular unsupervised use is a known cause of chronic kidney injury.
Ayurvedic and herbal supplements Certain Ayurvedic formulations containing heavy metals have documented kidney-damaging potential. If you are on long-term supplements, tell your doctor.
How Often Should You Get a KFT?
Group
Recommended Frequency
Healthy adult, no risk factors, normal past KFT
Once every 2-3 years
Diabetes, hypertension, obesity, family history of kidney disease
Every 6-12 months
Kidney stones, recurrent UTIs, high uric acid
Every 6-12 months
Long-term NSAID, herbal supplement, or antibiotic use
At least annually, or as advised
Known CKD or abnormal baseline KFT
As per nephrologist’s guidance
👩⚕️ Doctor’s Note A single mildly abnormal KFT value is not a diagnosis of kidney disease. Creatinine can rise after a hard gym session. BUN climbs after a protein-heavy meal. Calcium fluctuates with hydration and Vitamin D status. What your doctor looks for is a pattern across time, not a single number in isolation. If your results are borderline and you had any of the confounding factors discussed above, a repeat test after rest, good hydration, and a normal diet is usually the right first step.
When Should You Be Concerned? Speak to your doctor promptly if you notice any of the following:
Creatinine consistently above 1.4 mg/dL (men) or 1.2 mg/dL (women), especially if rising across two or more tests
BUN/Creatinine ratio above 23, paired with symptoms like excessive thirst, reduced urine output, or dizziness
Uric acid above 7.2 mg/dL with joint swelling, joint pain, or a history of kidney stones
Low calcium with muscle cramps, tingling in fingers, or persistent fatigue
Any KFT abnormality paired with visible symptoms: leg swelling, frothy urine, reduced urine output, persistent lower back pain
Always bring your actual report to your appointment – your doctor needs the specific values and your lab’s reference range, not a verbal summary
The Takeaway
Your kidneys are working every minute of every day – filtering, balancing, and regulating – and most of the time you feel nothing at all.
The KFT is one of the simplest ways to check that this work is still being done well. Understanding what BUN, creatinine, urea, uric acid, and calcium actually measure means you are no longer staring at numbers that mean nothing. It means you walk into your doctor’s appointment informed, with the right questions ready.
And that is exactly where better health starts.
Questions to Ask Your Doctor
My creatinine is slightly elevated – could it be related to dehydration or exercise before the test?
Should we repeat the KFT in two to three weeks to confirm the result?
Is my eGFR within normal limits for my age?
Given my diabetes or blood pressure, how often should I be getting a KFT done?
My uric acid is borderline high – is a diet change enough, or do I need medication?
Are any of my current medications, including supplements, affecting my kidney function?
References
Fauci AS et al. Harrison’s Principles of Internal Medicine, 21st Edition. McGraw-Hill Education.
Kumar V et al. Robbins and Cotran Pathologic Basis of Disease, 10th Edition. Elsevier.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice




: Purpose & Results")
Leave a Reply