An abnormal lipid profile — high cholesterol, high LDL, low HDL, elevated triglycerides — is among the most common findings in routine blood work in India today. This guide covers how to control cholesterol through diet, lifestyle, and medication.
Urban dietary shifts, sedentary jobs, chronic stress, and widespread Vitamin D and B12 deficiency have made dyslipidemia (abnormal lipid profile) a silent epidemic affecting millions of Indians across all age groups.
The most important truth: in most cases, lifestyle is both the cause and the cure. This article is a detailed, evidence-based guide to what actually moves the needle — with a specific focus on the Indian dietary context — followed by a clear summary of when medical treatment is warranted.
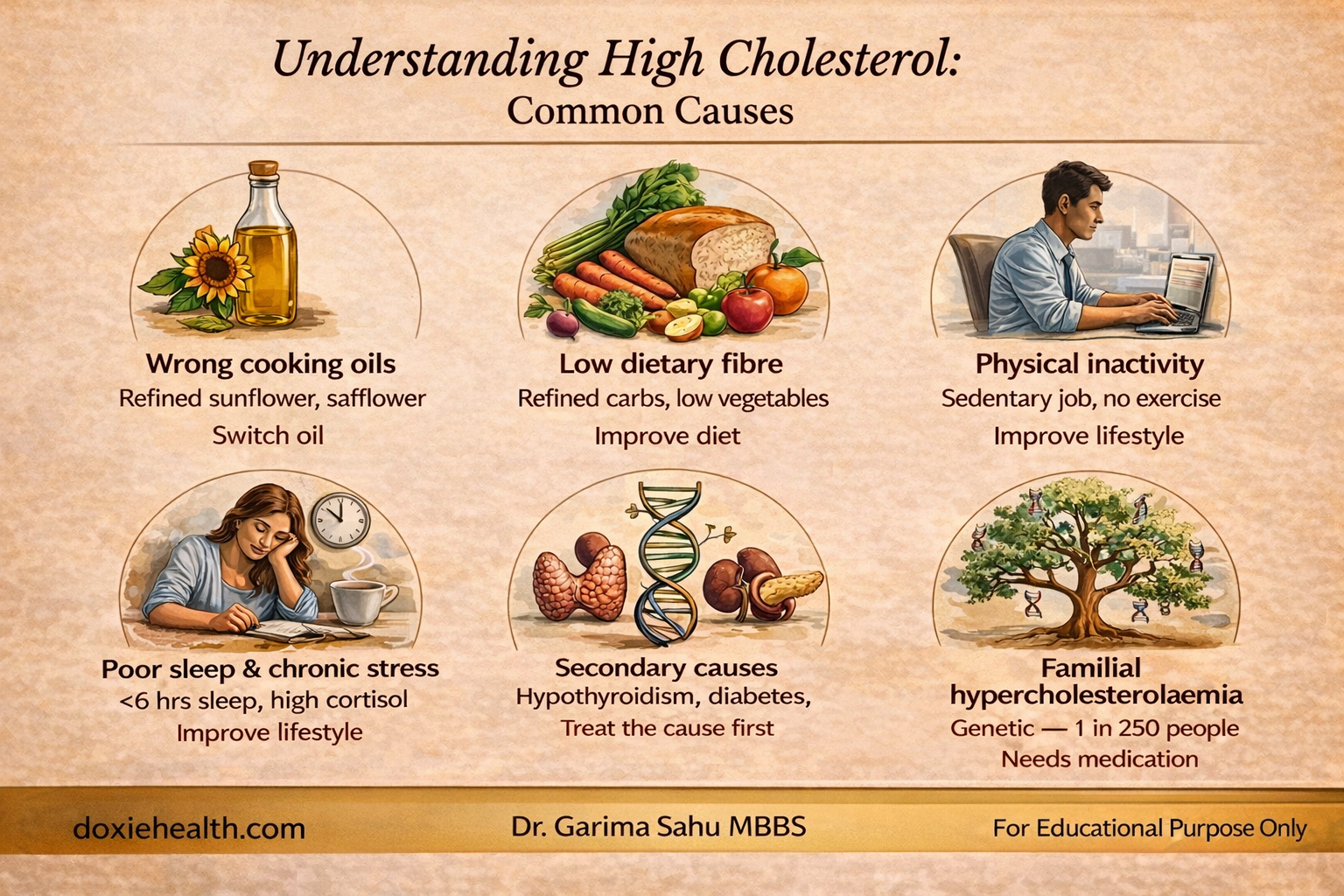
Lipid abnormalities are almost always multifactorial. Key drivers:
Common lifestyle, medical, and genetic causes of high cholesterol explained visually — DoxieHealth.
Key point: Always rule out a secondary cause first — particularly thyroid disease or uncontrolled diabetes. Treating the underlying condition can normalize lipid values without any additional intervention.
Smoking and Alcohol: Their Impact on Your Lipid Profile
Smoking lowers HDL and damages artery walls — even light smoking has a measurable impact. Quitting can raise HDL within weeks.
Excess alcohol is a leading cause of high triglycerides. The liver prioritizes alcohol over fat clearance, leading to triglyceride accumulation. Heavy drinking worsens the overall lipid profile.
Red wine contains resveratrol with modest anti-inflammatory properties, but real-world amounts are far below research doses. One small glass daily may be low-risk — beyond that, triglyceride-raising effects outweigh any benefit.
How to Control High Cholesterol: Lifestyle Changes That Work
The Oil Question — The Most Misunderstood Part of the Indian Diet
No dietary factor affects Indian lipid health more than cooking oil. Most Indian households switched to refined sunflower or soybean oil in the 1980s — both are extremely high in omega-6 PUFA, which promotes chronic inflammation when omega-3 intake is low.
Understanding Cooking Oils in Simple Terms
Dietary fats fall into three main types:
Saturated fats (solid at room temperature)- found in Ghee, Coconut Oil
Monounsaturated fats (MUFA) – found in oils like mustard and olive oil
Polyunsaturated fats (PUFA) – found in sunflower, safflower, soybean, and corn oil
Sesame oil — predominantly PUFA (linoleic acid, omega-6), with a significant MUFA component (oleic acid). It’s a mixed oil, but PUFA dominates. Peanut oil — predominantly MUFA (oleic acid), with a moderate PUFA content. Closer to the MUFA category — similar profile to olive oil but less oleic acid. Both are considered heart-neutral to mildly beneficial compared to saturated fats, but neither matches the MUFA dominance of olive or mustard oil. Those with gastritis or acidity may tolerate yellow mustard oil better than black.
The omega-6 problem: Your body needs omega-6 and omega-3 fats in balance, ideally at a 4:1 ratio or lower. Most Indians are already far over this limit, with an estimated ratio of 15:1 to 50:1. Refined sunflower oil makes it worse — its ratio is roughly 300:1. This excess omega-6 drives low-grade chronic inflammation, quietly increasing cardiovascular risk. Choosing cold-pressed over refined preserves more nutrients — but does not fix the imbalance. The ratio stays the same.
Why MUFA oils are better for daily cooking MUFA-rich oils like mustard and olive oil are more heat-stable, less prone to oxidation, and help improve lipid profile by supporting healthy HDL and lowering harmful LDL.
Bottom line: For regular Indian cooking, MUFA-rich oils are a healthier choice than PUFA-heavy oils like sunflower oil.
Rice bran oil: balanced MUFA/PUFA, contains oryzanol, which lowers LDL.
Cold-Pressed vs Refined Oils — Why It Matters
Cold-pressed (kachi ghani) oils are extracted mechanically without heat. They retain polyphenols, tocopherols (Vitamin E), and natural antioxidants that protect both the oil and the consumer.
Refined oils are processed with heat, chemicals, and bleaching. This extends shelf life but destroys protective compounds and produces oxidation byproducts even before the oil reaches your pan. Where possible, choose cold-pressed over refined — especially for low-heat cooking and salad dressings.
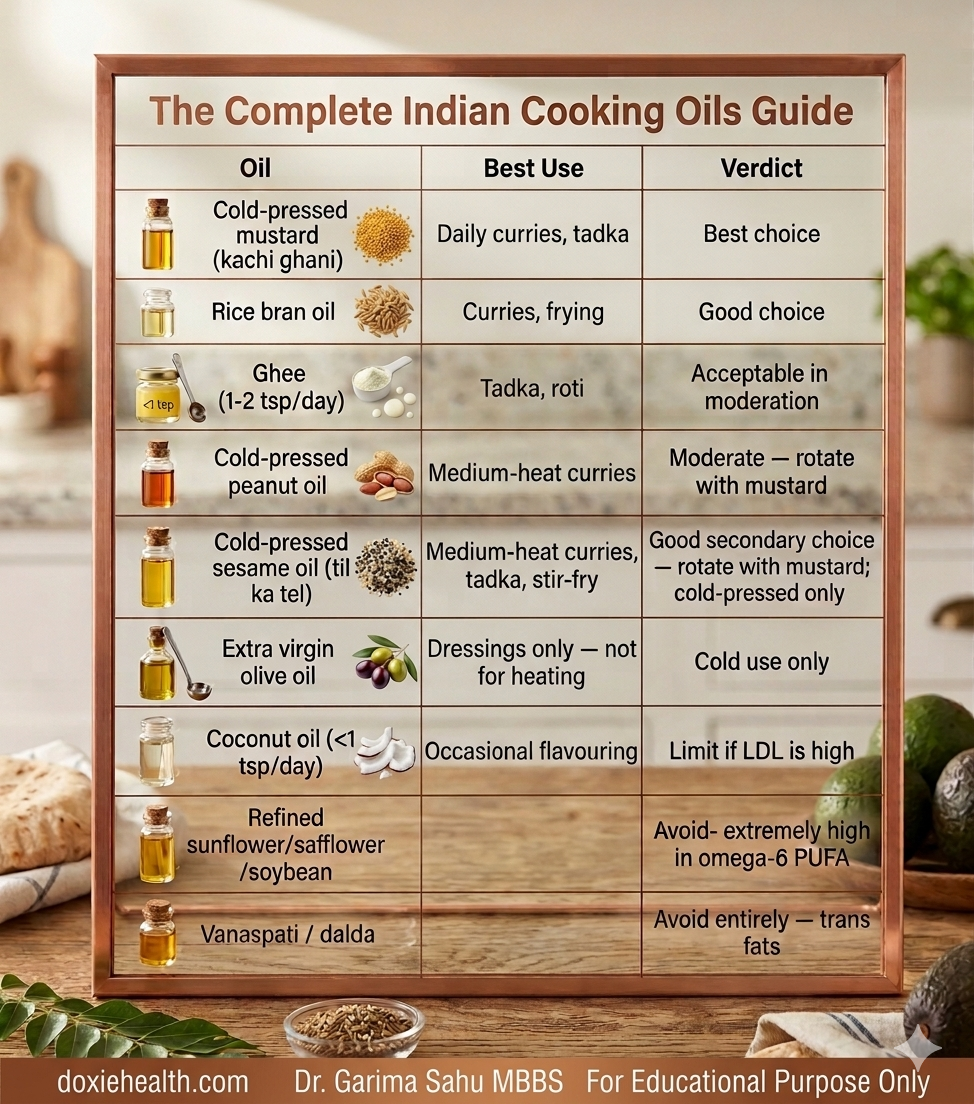
Cooking oil guide for managing high cholesterol in India — best and worst oils.Image: DoxieHealth
Ghee Ghee is predominantly saturated fat, but it contains short-chain and medium-chain fatty acids that are metabolised differently from long-chain saturated fats found in meat.
Traditional use in small amounts — 1 to 2 teaspoons per day for a healthy adult — is considered acceptable and does not appear to significantly worsen lipid profiles when the overall dietary pattern is sound.
If your LDL is already high, restrict to 1 teaspoon daily. Ghee used for tempering dal or roti is culturally practical and need not be eliminated — it should be moderated.
Coconut Oil Coconut oil is high in saturated fat but predominantly MCT (medium-chain triglycerides), which raises both LDL and HDL. Its net effect on cardiovascular risk remains debated. It is not recommended as your primary cooking oil if you have dyslipidaemia. If used, limit to 1 teaspoon per day. It is better suited as an occasional flavouring than a daily cooking medium.
Frying tip For Indian frying, use mustard oil or rice bran oil. Never reuse heated oil — repeated heating oxidises even stable oils and produces harmful aldehydes.
Dietary fibre — the underused cholesterol treatment
Dietary fibre is one of the most evidence-backed, cost-effective tools forlowering LDL — and most Indians are significantly under-consuming it.
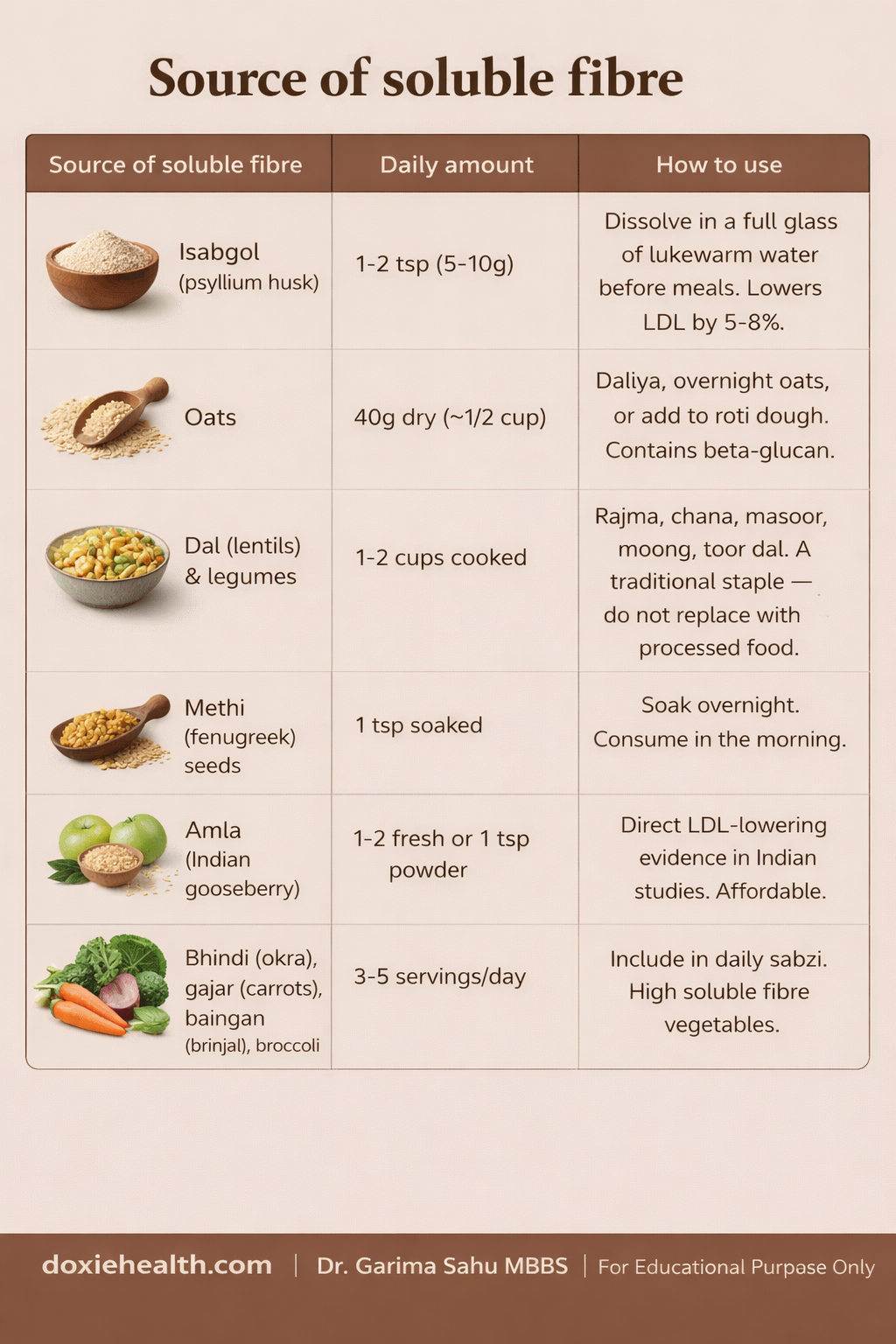
Soluble fibre binds to bile acids (which are made from cholesterol), preventing their reabsorption and forcing the liver to use up more circulating LDL cholesterol to make new bile.
Simple guide to daily soluble fibre sources and how to include them in your routine for better cholesterol and metabolic health. Doxiehealth
Nuts and seeds — with practical quantities
Nuts are one of the most consistently beneficial dietary additions for lipid health — but quantities matter.
Daily nut and seed guide infographic showing recommended portions of walnuts, almonds, flaxseeds, chia seeds, and pumpkin seeds for heart health. Doxiehealth
Note on cashews: Limit cashews — higher saturated fat than other nuts. Avoid commercially salted or roasted nut mixes (excess sodium and unhealthy oils).
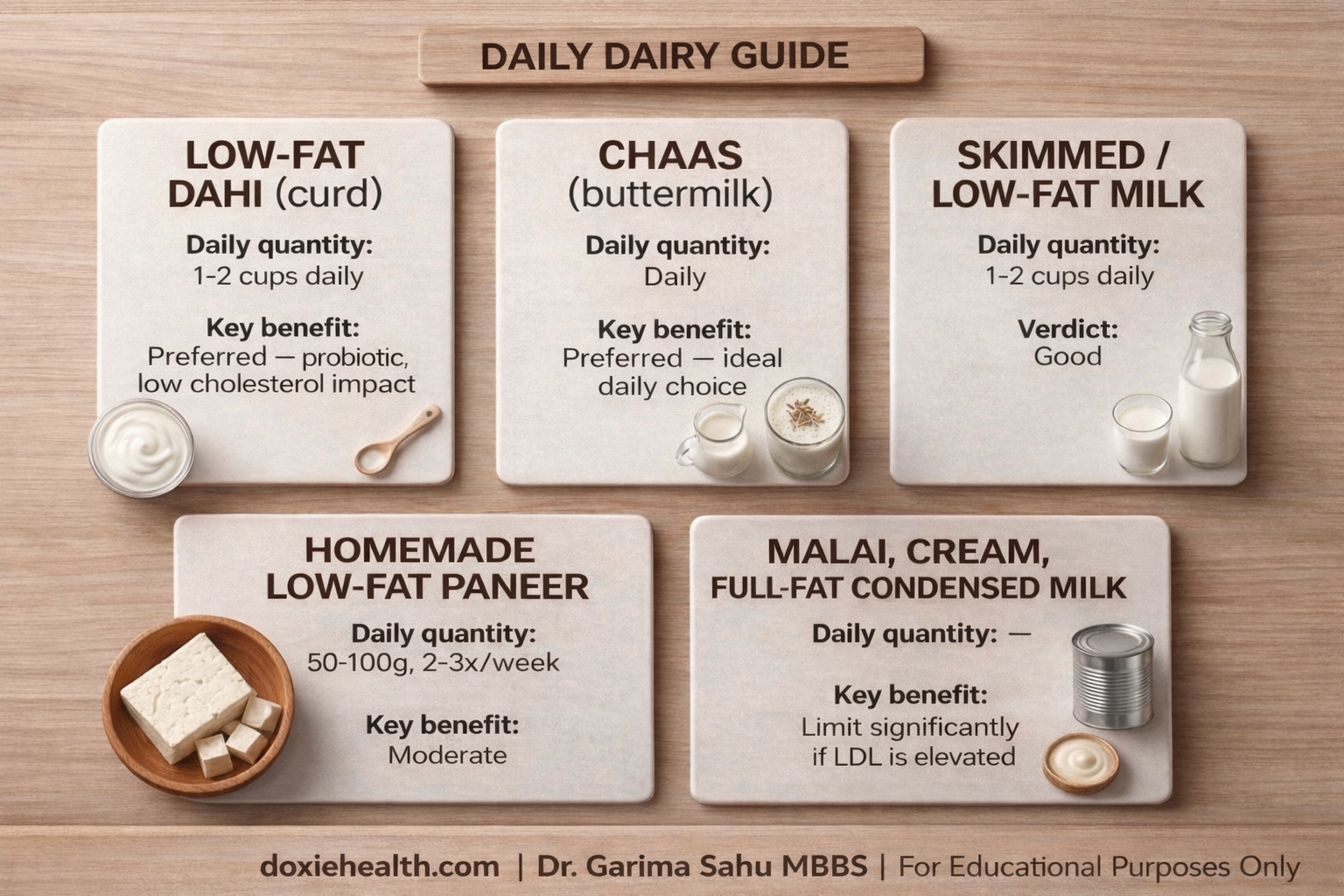
Dairy in the Indian context
Daily dairy guide for heart health: choose low-fat curd, chaas, and milk regularly, enjoy homemade low-fat paneer in moderation, and limit cream and condensed milk. Doxiehealth
Vitamin D and B12 — the missing links
Vitamin D: Despite abundant sunlight, Vitamin D deficiency is paradoxically widespread in India — affecting an estimated 70-90% of the urban population, largely due to indoor lifestyles, darker skin requiring longer sun exposure, and air pollution blocking UVB rays.
Vitamin D deficiency is independently associated with lower HDL, higher triglycerides, and insulin resistance.
Vitamin D and cholesterol are closely connected. Learn more in our complete guide to Vitamin D deficiency, symptoms, and treatment:
Practical steps: 15 to 20 minutes of direct midday sun (10 am-2 pm) on arms and legs, most days of the week. If your 25-OH Vitamin D level is below 30 ng/mL, supplementation is required as guided by your doctor.
Vitamin B12
B12 deficiency is extremely prevalent among Indian vegetarians. Low B12 raises homocysteine, which directly damages artery walls, compounding the cardiovascular risk from dyslipidemia independently of LDL levels.
Action: A B12 below 300 pg/mL warrants supplementation. Vegetarians almost always require supplementation — either oral cyanocobalamin or methylcobalamin. Your doctor will advise on the dose and frequency based on your level.
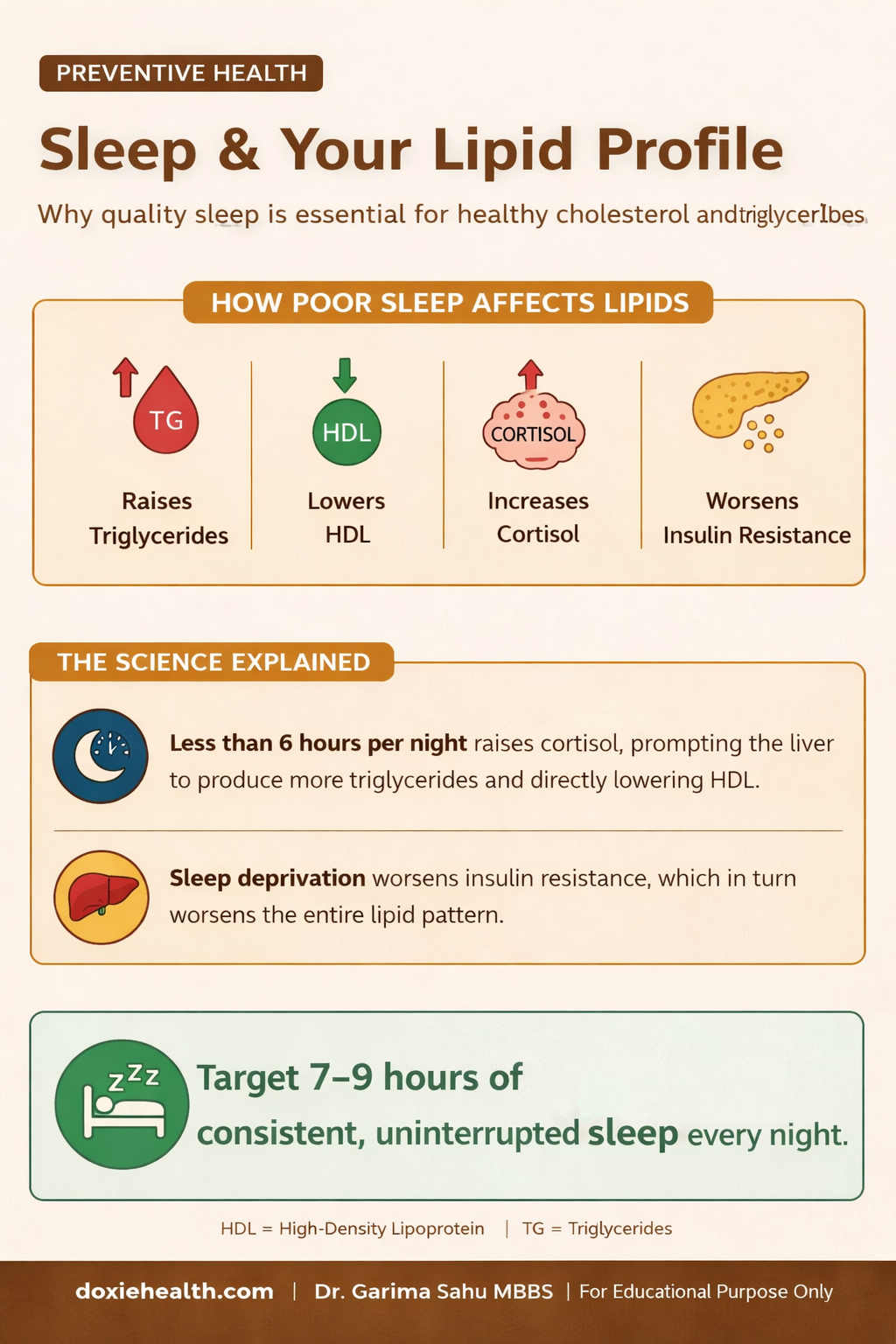
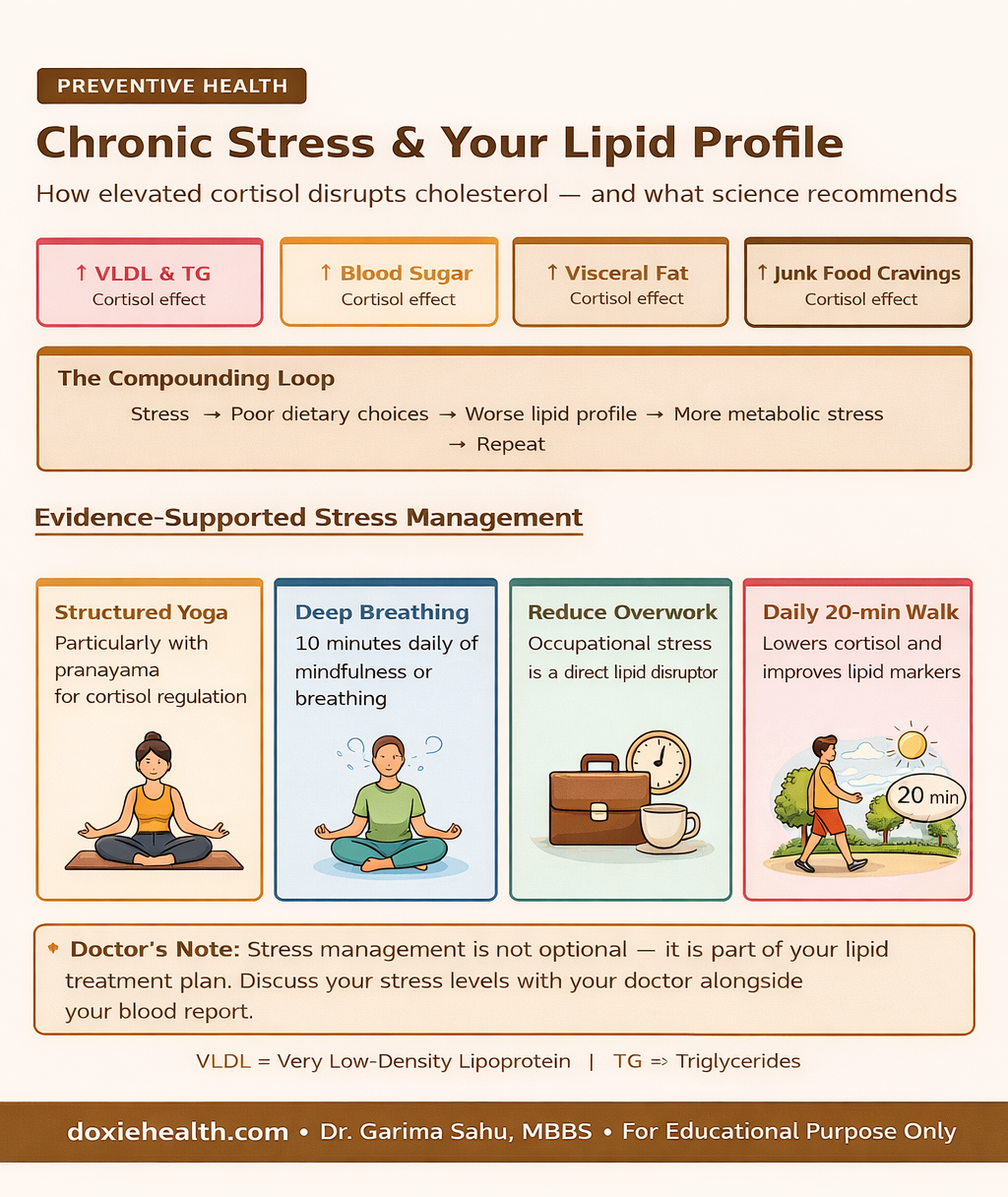
Sleep and stress
Sleep: Chronic poor sleep is a direct metabolic disruptor.
Obstructive sleep apnoea: loud snoring, interrupted sleep, daytime fatigue -is strongly linked to dyslipidemia and significantly underdiagnosed in India.
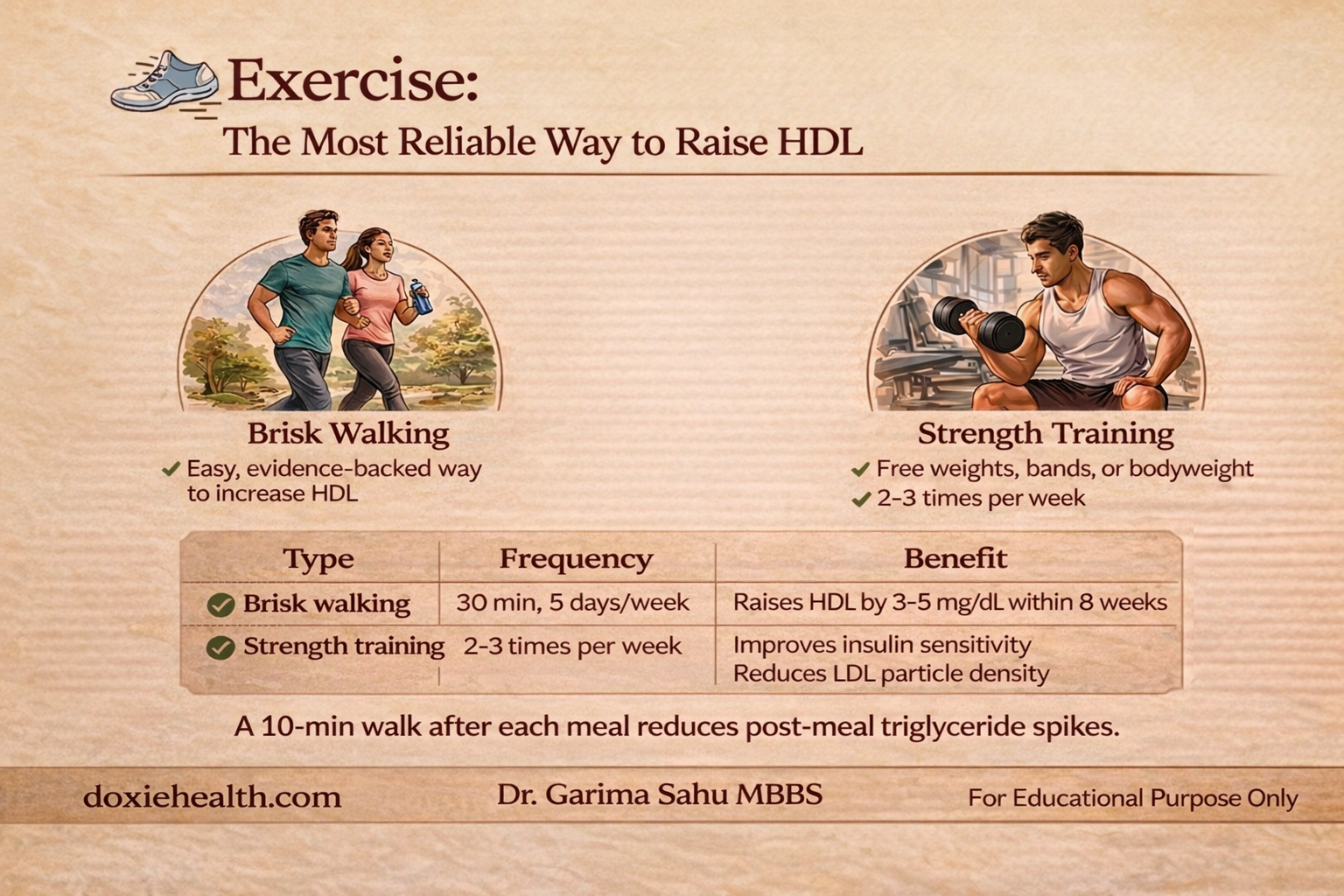
Exercise is one of the most reliable ways to raise HDL: brisk walking for 30 minutes 5 days a week and strength training 2–3 times a week improve insulin sensitivity and support healthier cholesterol levels.
Brisk Walking
The single most accessible and evidence-backed exercise for lipid improvement.
Pace matters: brisk means you can speak in short sentences but cannot sing comfortably.
Strength Training
Bodyweight exercises, free weights, or resistance bands — improve insulin sensitivity and reduce LDL particle density (making LDL particles larger and less atherogenic, even when total LDL count does not change dramatically).
Key principle: Consistency matters more than intensity. Combine aerobic and resistance training for the best lipid outcomes. A sustainable 30-minute daily routine delivers far more long-term cardiovascular benefit than sporadic high-intensity sessions.
Medical management (when lifestyle is not enough)
Medication is considered when LDL remains significantly elevated after 3-6 months of genuine lifestyle effort, when cardiovascular risk is already high, or when familial hypercholesterolemia is present.
Medication
Primary action
Used for
Statins (atorvastatin, rosuvastatin)
Inhibit hepatic cholesterol production
First-line for high LDL. Most evidence-backed class.
Fibrates (fenofibrate)
Lower triglycerides, raise HDL
High triglycerides or low HDL as dominant concern
Ezetimibe
Blocks intestinal cholesterol absorption
Added to statin for further LDL reduction
Nicotinic acid (Niacin)
Most effective agent for raising HDL
Persistently low HDL or high triglycerides. May cause flushing.
Pyridoxine (Vitamin B6)
Homocysteine lowering (with B12 + folate)
Elevated homocysteine — especially in vegetarians with B12 deficiency
Omega-3 prescription (EPA)
Lowers very high triglycerides
Triglycerides above 500 mg/dL (pancreatitis risk)
PCSK9 inhibitors
Injectable — dramatic LDL reduction
Very high-risk patients or familial hypercholesterolaemia
Important Medication and lifestyle are not either/or. The evidence strongly supports combining both. Statins only protect when taken consistently — irregular use negates most cardiovascular benefit.
👩⚕️ Doctor’s Note An abnormal lipid profile in an Indian patient is almost never about one thing. It is usually the sum of dietary choices accumulated over decades, low fibre intake, inadequate Vitamin D and B12, disrupted sleep, and chronic stress. Address the full picture — not just the number on the report.
When to see your doctor promptly LDL above 190 mg/dL despite sustained lifestyle changes Triglycerides above 500 mg/dL Family history of heart attack before age 55 (men) or 65 (women) Unexplained muscle pain on a statin No improvement after 3-6 months of consistent effort
The Takeaway
Dyslipidemia in the Indian context is driven by a specific and identifiable cluster of lifestyle factors — the wrong food choices, cooking oils, insufficient fibre, inadequate Vitamin D and B12, poor sleep, and physical inactivity.
Each of these is modifiable. Address them systematically, track your lipid profile every 3-6 months, and work with your doctor on whether medication adds benefit to your specific risk profile.
Questions to Ask Your Doctor
What is my calculated 10-year cardiovascular risk – not just my cholesterol number?
Should I check my Vitamin D, B12, homocysteine, and thyroid levels?
Is isabgol appropriate for me alongside dietary changes?
Should I start medication now or try lifestyle changes first with a 3-month review?
If prescribed a statin, what muscle symptoms should prompt me to call you?
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice


 Explained")


Leave a Reply