High cholesterol is becoming surprisingly common among young adults today. If you’ve recently checked your lipid profile and weren’t quite sure how to interpret the numbers, it’s completely understandable.
The good news is — this is something you can understand and manage. Before jumping to solutions, it helps to first know what high cholesterol actually means, why it rises, and how simple changes can make a real difference.
A lipid profile — also called a lipid panel or cholesterol test — is a blood test that measures the fats circulating in your bloodstream.
These fats play essential roles in the body, but when they fall out of balance, they can silently damage blood vessels and raise your risk of heart disease over many years.
Think of your bloodstream as a delivery network. Cholesterol and fats are constantly being transported — from your liver to your tissues and back.
The lipid profile tells you how much of each type is in circulation, and whether the balance is healthy.
The test should always be done fasting — 9 to 12 hours without food — because eating temporarily raises triglyceride levels and distorts results.
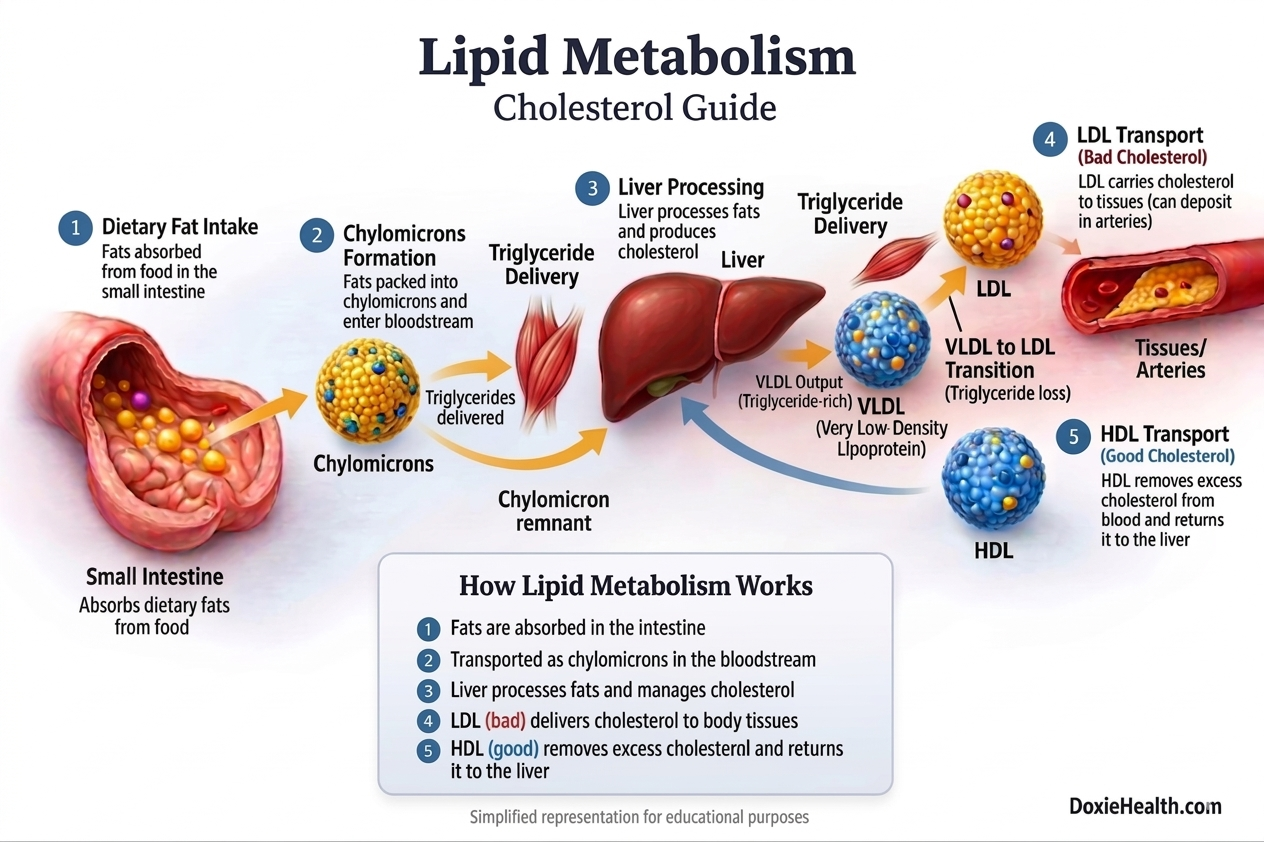
Lipid Metabolism — How Fats Travel in Your Body
How lipid metabolism works — from food to your arteries. Image: DoxieHealth
After a meal, your small intestine absorbs dietary fats. However, these fats cannot be used directly by the body. They must first be digested, packaged, and transported so they can either be used for energy or stored for later use.
Because lipids are not water-soluble, they cannot travel freely in the bloodstream. To solve this, the body uses specialized “transport particles” called lipoproteins (lipid+Protein) to carry triglycerides and cholesterol through the blood.
Each type of lipoprotein has a specific role:
Chylomicrons → carry dietary fats (Mainly triglycerides) from the small intestine to the body
VLDL → LDL → deliver triglycerides and cholesterol to the body
HDL → removes excess cholesterol from blood stream and returns it to the liver
Let’s understand this step by step in a simple way.
Absorption from the Small Intestine
After digestion, fats are absorbed in the small intestine. These fats are mainly in the form of triglycerides, along with a small amount of cholesterol.
Since fats cannot travel freely in the blood, the body packages them into tiny particles called chylomicrons, which enter the bloodstream through the lymphatic system.
These act as the first transport vehicles carrying fats from your diet.
Delivery of Energy to Tissues
Chylomicrons travel through the bloodstream and deliver triglycerides (energy) to:
Muscles (for immediate use)
Fat tissue/adipose tissue (for storage)
After delivering most of their triglycerides, the remaining particles (called chylomicron remnants) are taken up by the liver.
The Liver — The Central Processing Unit
The liver plays a central role in lipid metabolism. Nearly 80% of the cholesterol in the body is produced by the liver, while the remaining portion comes from the diet.
Along with producing cholesterol, the liver also repackages fats into VLDL (Very Low-Density Lipoprotein).
These particles primarily carry triglycerides, along with a smaller amount of cholesterol, into the bloodstream.
From VLDL to LDL
As VLDL circulates, it delivers triglycerides to tissues. As it loses these triglycerides, it gradually transforms into LDL (Low-Density Lipoprotein).
LDL is richer in cholesterol and primarily delivers it to body cells.
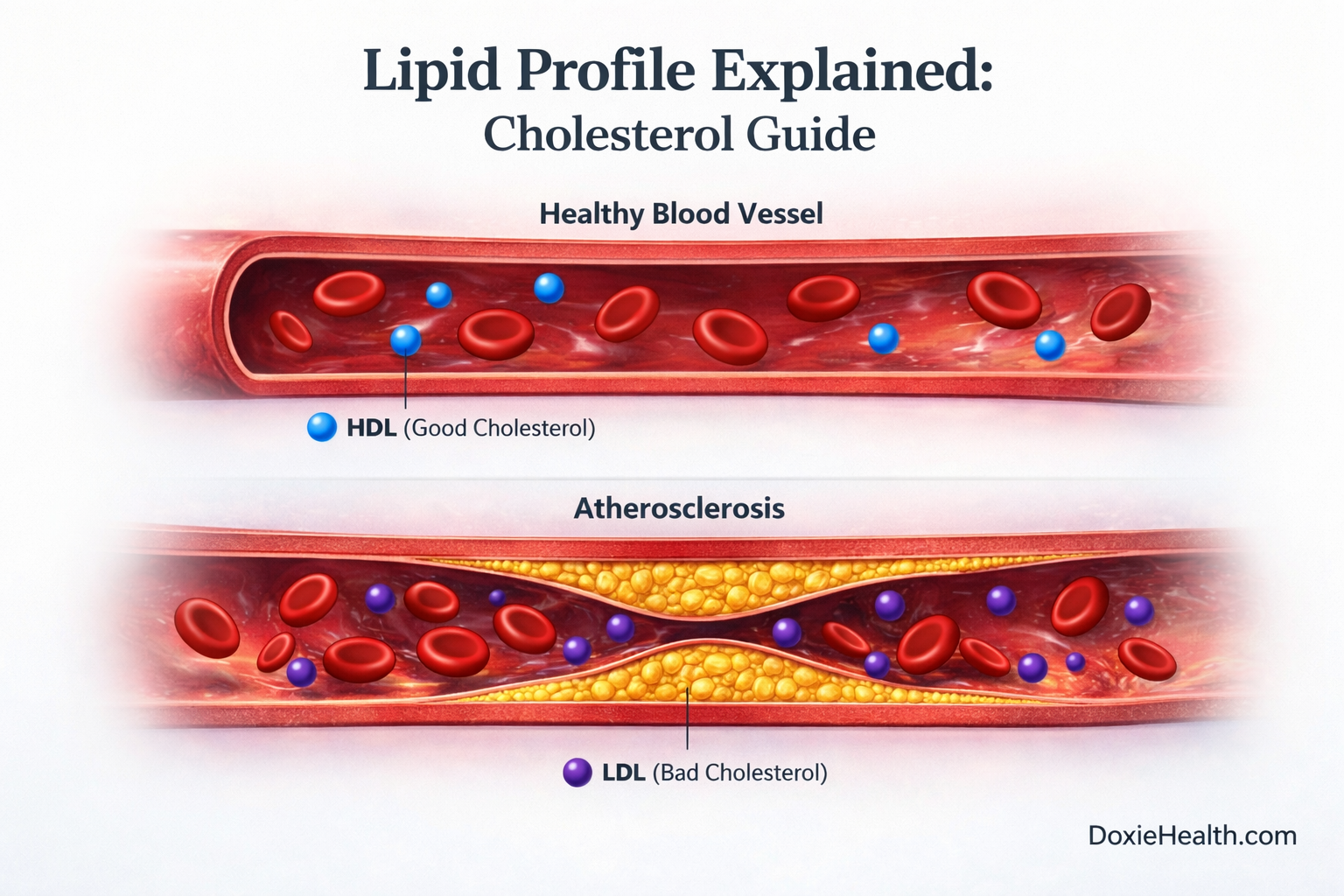
When LDL Becomes a Problem
In normal amounts, LDL is useful. But when LDL levels are high, excess cholesterol can start depositing in artery walls. Over time, this can lead to plaque formation, a process known as Atherosclerosis.
HDL — The Cleanup System
To balance this, the body uses HDL (High-Density Lipoprotein).
HDL collects excess cholesterol from the bloodstream and transports it back to the liver for removal. This protective process is known as reverse cholesterol transport.
Simple Takeaway VLDL, LDL, and HDL are lipoproteins — transporters that carry lipids (triglycerides and cholesterol) in the blood. LDL delivers cholesterol outward. HDL brings it back. The balance between the two determines your long-term cardiovascular risk.
Quick Reference: Normal Lipid Profile Ranges
Standard adult reference ranges. Your lab report may show slightly different values.
Marker
Optimal
Borderline
High Risk
Total Cholesterol
Below 200 mg/dL
200–239 mg/dL
240+ mg/dL
LDL Cholesterol
Below 100 mg/dL
130–159 mg/dL
160+ mg/dL
HDL Cholesterol
Above 60 mg/dL ✓
40–59 mg/dL
Below 40 mg/dL
Triglycerides
Below 150 mg/dL
150–199 mg/dL
200+ mg/dL
Non-HDL Cholesterol
Below 130 mg/dL
130–159 mg/dL
160+ mg/dL
VLDL Cholesterol
2–30 mg/dL
—
Above 30 mg/dL
TC/HDL Ratio
Below 3.5
3.5–5.0
Above 5.0
LDL/HDL Ratio
Below 2.5
2.5–3.5
Above 3.5
For HDL — higher is better. It is the only marker where a low value is the concern.
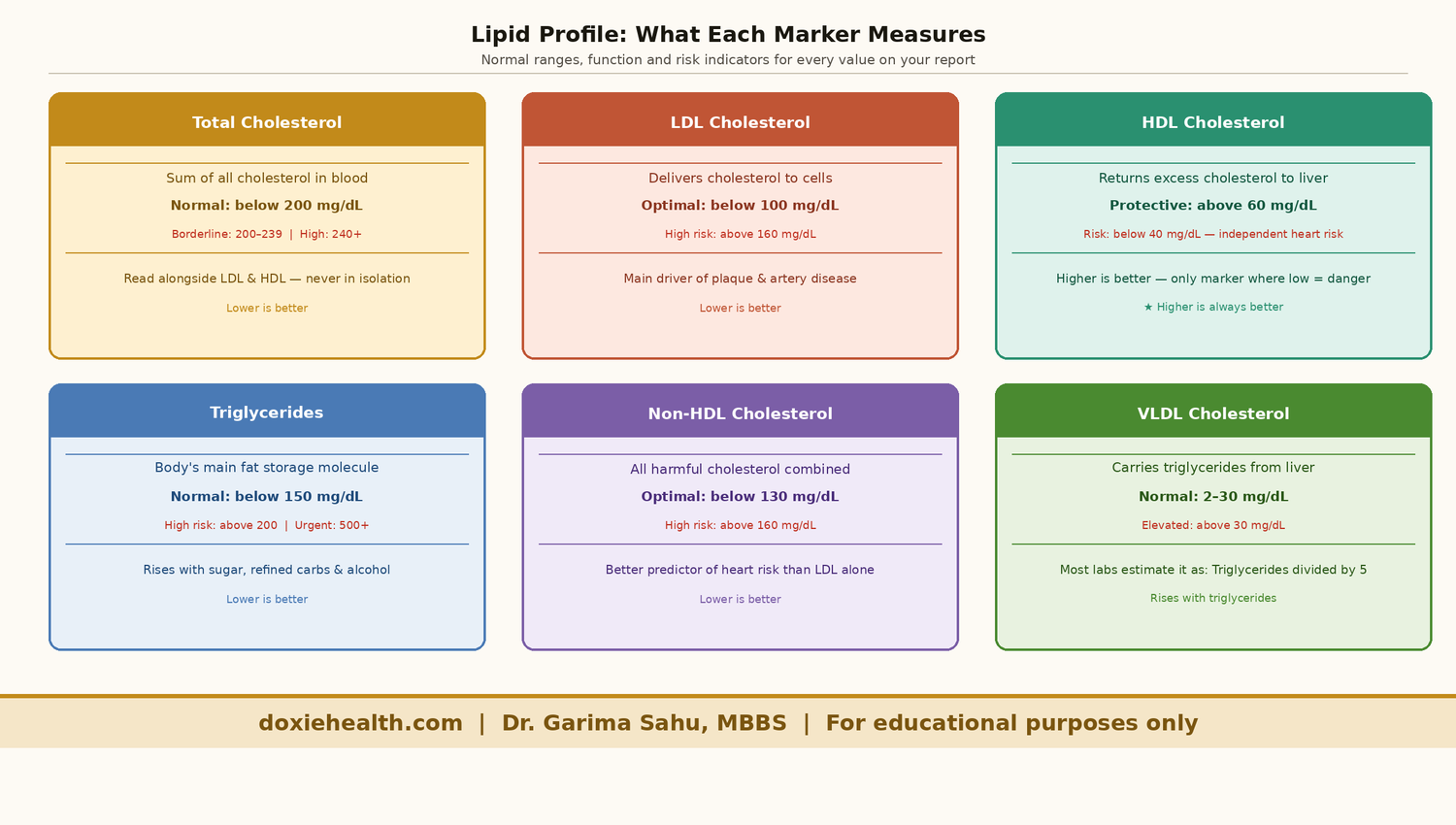
Lipid Profile Markers
All lipid profile markers explained at a glance. Diagram: DoxieHealth
Total Cholesterol
It is the first number most people look at, but also the most misleading when read in isolation.
This does not represent all the cholesterol in your body. Instead, it reflects the amount of cholesterol present in your bloodstream at that moment.
Total cholesterol is the sum of all cholesterol types in your blood carried by different lipoproteins:
Total Cholesterol ≈ LDL + HDL + VLDL
Why Total Cholesterol Alone Is Not Enough
Total cholesterol doesn’t tell the full story. Two people can have the same value but very different risk levels depending on their LDL and HDL.
High LDL + low HDL → higher risk
Low LDL + high HDL → lower risk
For example, a total cholesterol of 220 mg/dL could mean either unhealthy LDL levels or simply high HDL. That’s why the breakdown matters more than the total cholesterol alone. This is why total cholesterol is always read alongside the breakdown.
Causes of high total cholesterol:
Diet: high saturated fat intake — ghee, butter, red meat, full-fat dairy
Lifestyle: physical inactivity, obesity, smoking
Hypothyroidism: one of the most common and underdiagnosed causes — the thyroid hormone regulates how the liver processes cholesterol, so even a mildly underactive thyroid can cause a significant rise in total cholesterol and LDL. Always check TSH if cholesterol is unexpectedly high
Other medical causes: kidney disease, uncontrolled diabetes, and certain medications such as steroids
Genetics: familial hypercholesterolaemia — inherited high LDL from birth
Complications: Persistently high total cholesterol drives atherosclerosis- the gradual build-up of fatty plaques inside artery walls -which raises the risk of heart attack, stroke, and peripheral artery disease over time.
Cholesterol is not simply a harmful substance — it is essential. Your body uses it to build cell membranes, produce hormones like oestrogen and testosterone, synthesise Vitamin D, and make bile acids for digestion. Total cholesterol shows how much cholesterol is present in your blood, but not how it is distributed.
LDL Cholesterol — Direct
LDL (Low-Density Lipoprotein) is the primary carrier of cholesterol from the liver to the rest of the body.
When LDL levels are too high, excess cholesterol is deposited into artery walls, forming plaques — a process called atherosclerosis. It is the single most important number on your lipid profile.
Your report says LDL — Direct, meaning it was measured directly in the lab rather than estimated using a formula. Direct measurement is more accurate — particularly when triglycerides are elevated above 200 mg/dL.
Causes of high LDL:
Diet: high saturated fat intake — ghee, butter, red meat, full-fat dairy
Lifestyle: physical inactivity, obesity, smoking
Hypothyroidism: one of the most common and underdiagnosed causes.
Other medical causes: uncontrolled diabetes
Genetics: familial hypercholesterolaemia — inherited high LDL from birth
Certain cholesterol-lowering medications (statins, ezetimibe)
Rare inherited conditions — abetalipoproteinaemia
LDL targets depend on your overall risk:
Healthy adult with no risk factors — below 130 mg/dL
Person with diabetes or hypertension — below 100 mg/dL
Person with known heart disease — below 70 mg/dL
HDL Cholesterol — Direct
HDL (High-Density Lipoprotein) works in the opposite direction to LDL. It collects excess cholesterol from artery walls and transports it back to the liver for removal — a process called reverse cholesterol transport.
HDL is the only marker on your lipid profile where higher is better.
Causes of low HDL:
Physical inactivity — the single most common cause in Indian adults
Smoking directly reduces HDL levels
Obesity — particularly abdominal obesity
High refined carbohydrate diet — white rice, bread, sugary drinks
Type 2 diabetes and insulin resistance
Metabolic syndrome
Complications of low HDL:
An HDL below 40 mg/dL is an independent risk factor for heart disease — even when LDL appears completely normal.
Low HDL below 40 mg/dL in men and below 50 mg/dL in women significantly raises cardiovascular risk.
High HDL: Regular aerobic exercise, healthy fats (olive oil, nuts, fatty fish), stopping smoking, and certain genetic variants.
High HDL is generally protective and rarely a concern.
Triglycerides
Triglycerides are your body’s main fat storage molecule — think of them as a fuel reserve. When you consume more calories than you burn, particularly from sugar and refined carbohydrates, the excess is converted into triglycerides and stored in fat cells for later use.
When persistently elevated, they contribute to cardiovascular risk and are strongly linked to metabolic syndrome, fatty liver disease, and insulin resistance.
Causes of high triglycerides:
High sugar and refined carbohydrate intake — white rice, bread, sugary drinks
Alcohol — even moderate amounts significantly raise triglycerides
Physical inactivity
Uncontrolled diabetes
Hypothyroidism
Certain medications — steroids, beta blockers, and oral contraceptives
Causes of low triglycerides: Malnutrition, hyperthyroidism, and very low-fat diets. Low triglycerides are rarely a clinical concern.
Important: Triglycerides must always be measured fasting. A non-fasting sample produces falsely elevated results. Additionally, triglycerides above 500 mg/dL carry a specific risk of acute pancreatitis — a serious complication requiring urgent medical attention.
Non-HDL Cholesterol
Non-HDL cholesterol is calculated as Total Cholesterol minus HDL. It captures all cholesterol carried by potentially harmful particles — LDL, VLDL, and IDL — in a single number.
Many cardiologists consider non-HDL cholesterol a better predictor of cardiovascular risk than LDL alone, because it accounts for all plaque-forming particles, not just LDL.
The target for most adults is below 130 mg/dL — 30 points higher than the LDL target.
Causes of high Non-HDL: Same as high LDL and high triglycerides — saturated fat intake, refined carbohydrates, physical inactivity, and metabolic dysfunction.
VLDL Cholesterol
VLDL (Very Low-Density Lipoprotein) is the liver’s primary transporter of triglycerides into the bloodstream.
It is closely linked to triglyceride levels — when triglycerides rise, VLDL typically rises with them. Normal range is 2–30 mg/dL.
VLDL contributes to plaque formation, though it is considered less harmful than LDL.
Most Indian labs calculate VLDL from triglycerides using the formula:
VLDL = Triglycerides ÷ 5
Elevated VLDL generally reflects elevated triglycerides and responds to the same lifestyle changes.
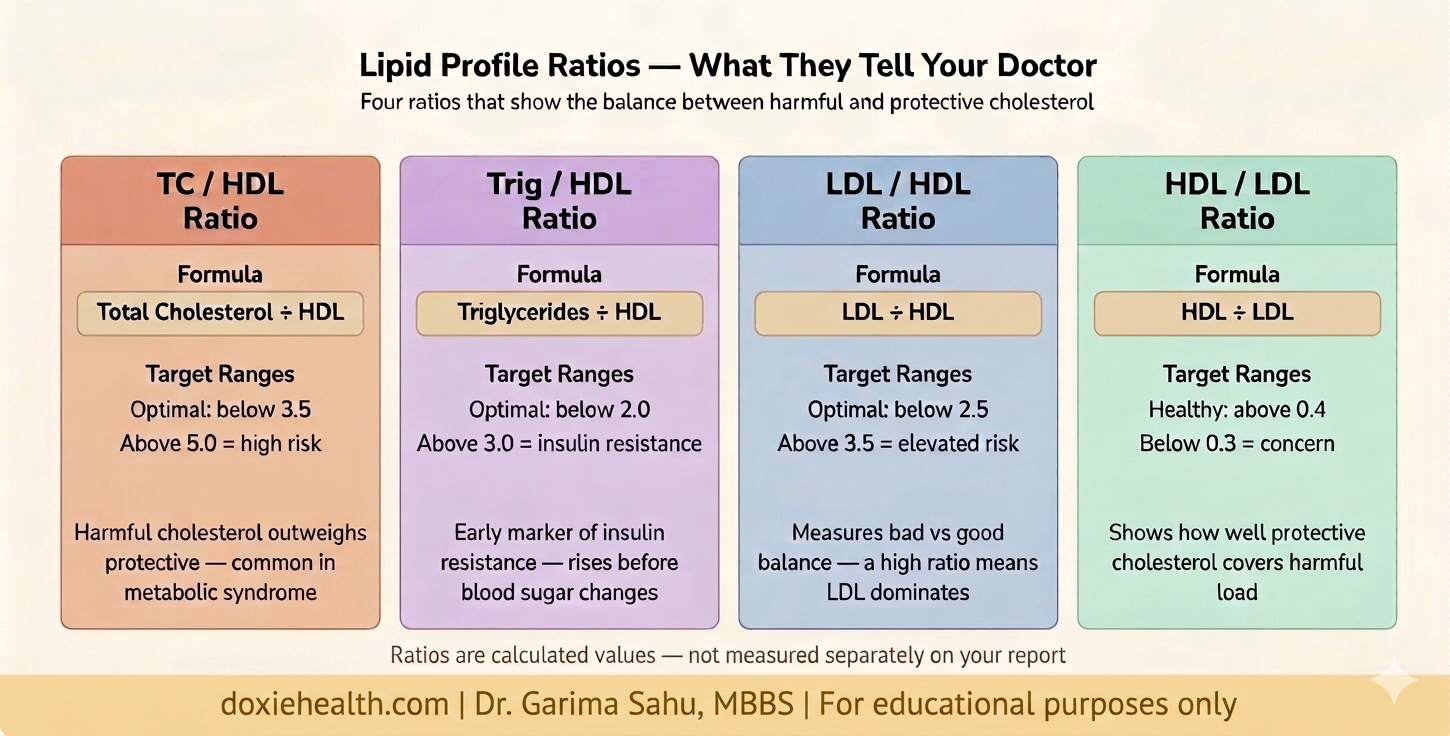
The Ratios — What They Add
Your lipid report includes four ratios. They are not independent markers — they are mathematical relationships between existing values. However, they give a quick snapshot of the balance between harmful and protective cholesterol.
Lipid profile ratios and what they mean for your heart health. Image: DoxieHealth
Key Clinical Insights
Never read total cholesterol alone — always look at LDL, HDL and triglycerides together as a pattern
Low HDL is as important as high LDL — an HDL below 40 mg/dL is an independent risk factor for heart disease
The Trig/HDL ratio is an underused early marker — a ratio above 3.0 suggests insulin resistance before glucose levels become abnormal
LDL — Direct is more accurate than calculated LDL — particularly when triglycerides are elevated above 200 mg/dL
A normal lipid profile does not completely rule out heart disease — additional markers such as hsCRP and Lp(a) provide further information
👩⚕️ Doctor’s Note The lipid profile is one of the most actionable blood tests in medicine — but numbers only make sense in context. A mildly raised LDL in a young, active person is not the same as the same number in someone with diabetes and high blood pressure. If your cholesterol is unexpectedly high, always check your thyroid first — hypothyroidism is a common and very treatable cause that is frequently missed. Always bring your full report to your appointment, not just the total cholesterol value.
When Should You Be Concerned?
Speak to your doctor promptly if:
LDL above 160 mg/dL — particularly with other risk factors such as diabetes or high blood pressure
HDL below 40 mg/dL — an independent risk factor regardless of LDL
TC/HDL ratio above 5.0 — suggests significant cardiovascular risk
Trig/HDL ratio above 3.0 — early marker of insulin resistance worth investigating
Family history of early heart disease — screen early and more frequently, regardless of current results
The Takeaway
Your lipid profile is a window into your long-term cardiovascular and metabolic health. Each marker tells a specific part of the story — and no single number gives the full picture.
LDL drives plaque build-up. HDL clears it. Triglycerides reflect your metabolic health. The ratios tell you how these markers relate to each other.
Understanding all of them helps you walk into your doctor’s appointment informed, calm, and ask the right questions.
Questions to Ask Your Doctor
“Am I at risk based on my full lipid profile, not just total cholesterol?” helps you understand your overall risk, not just one number
“What is my LDL target based on my overall risk profile?” The answer varies significantly between individuals
“Can I manage this with lifestyle changes, or do I need medication?” guides next steps
“What does my report suggest about my metabolic health?” a useful early screening question
“How often should I retest my lipid profile?” depends on current results and risk factors
“What specific diet or lifestyle changes will help my numbers?” makesadvice actionable
References & Further Reading
Kasper DL et al. Harrison’s Principles of Internal Medicine, 21st ed. McGraw-Hill, 2022.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional for guidance about your specific health situation.
WRITTEN & MEDICALLY REVIEWED BY
Dr. Garima Sahu, MBBS
Physician & Founder, DoxieHealth
This article is for educational purposes only and does not replace professional medical advice
 Explained")



Leave a Reply